Anatomy 101
Saturday, January 1, 12022 HE
A word of warning. My interest in anatomy started in high school when I got into strength training. Anatomy was then my favourite subject during my undergraduate degree in Human Kinetics. It remained my favourite subject during my Physical Therapy studies. It was still my favourite area of study when I completed a Diploma in Manual Osteopathy. All this is to say that this may go into too much detail for the less anatomically enthused.
Full disclosure, I am a licensed physical therapist and manual osteopathic practitioner, but the following is purely for informational purposes. For formal guidance concerning your stand up paddleboard (SUP) biomechanics, it may be in your interests to seek out the aid of a licensed/qualified professional. If you are experiencing pain with physical activity, exercise a degree of caution when evaluating the nature of your symptoms. Pain with movement or exertion can be a normal symptom, but it may also signal something more nefarious. Use your own personal judgement, but if in doubt, err on the side of caution for a proper evaluation licensed/qualified medical professional.
- Anatomy 101
- How Shoulders Took Over the World
- SUP Biomechanics Introduction
- Mobility and Stability Subsystems
- What’s in a Shoulder? Bones and Joints.
- Passive Stuff: Joint Type, Capsule, Ligaments, Labrum
- Active Stuff: The Neuromuscular System
- Movements
- The Plumbing: Vasculature and Lymphatics
This is my second post on SUP biomechanics. For my first, more general post, see here.
How Shoulders Took Over the World
SUP Biomechanics Introduction
Stand up paddleboarding is a quickly growing aquatic recreational and sporting activity. It is easily accessible to most people since it requires minimal equipment and is easy to learn. It can be practiced on almost any body of water and provides a low-impact, full-body physical challenge, suitable for all ages and skill levels. As with any activity, SUP has risks (see this post for general SUP safety guidelines). Concerning musculoskeletal injuries specifically, a 2017 study by Furness et al. revealed that the shoulder/upper arm was the most frequently injured body location (32.9% of all injuries), followed by the lower back (14.3%), and the elbow/forearm (11.8%). Sub-optimal paddling stroke biomechanics have previously been associated with injury. For anyone getting into paddling, particularly if you plan to endurance paddle, paying attention to your stroke mechanics is a consideration of concern. Endurance paddling has the potential to magnify any errors in paddling stroke due to the repetitive nature and volume of activity.
In 2019 Schram and colleagues compared the stroke biomechanics of experienced and inexperienced paddlers. The study’s main finding was that experienced SUPers used less shoulder movement and more hip movement. It is worth noting that the data was collected while participants paddled on a KayakPro SUP ergometer. Despite the device’s previous validation, it is likely not a carbon copy of the real world. But it provides some useful insights.
The video clip below is animations of two representative paddlers created from their biomechanical data. The experienced paddler on the left demonstrates much more full-body movement than the inexperienced paddler on the right.
But before we delve into the biomechanics of the shoulder during SUP, here is an anatomical overview of the shoulder and its general biomechanics (for more details, see Goetti et al., 2020 and Chang et al., 2021).
Mobility and Stability Subsystems
In 1992 Panjabi proposed his landmark theoretical model for spinal stability. Simply the model suggests that dynamic stabilization of an anatomical structure is achieved via the coordination of three subsystems (neural, passive, and active). This model can be applied to all the articulations in the body. Hoffman and Gabel (2013) expanded on Panjabi’s original model to highlight the expression of movement. Essentially, they proposed a stability and mobility division of Panjabi’s original three subsystems (see the images below). As will be covered, for the shoulder to function and be stable, there must be cooperation between the various subsystems contributing to mobility and stability.

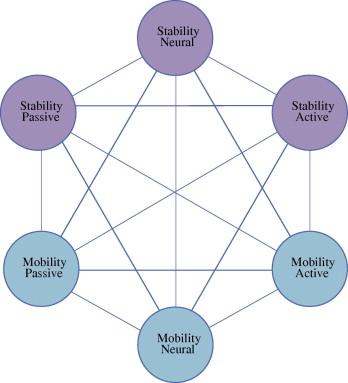
Source: Hoffman, J., and P. Gabel. “Expanding Panjabi’s Stability Model to Express Movement: A Theoretical Model.” Medical Hypotheses, vol. 80, no. 6, 2013, pp. 692–697., https://doi.org/10.1016/j.mehy.2013.02.006.
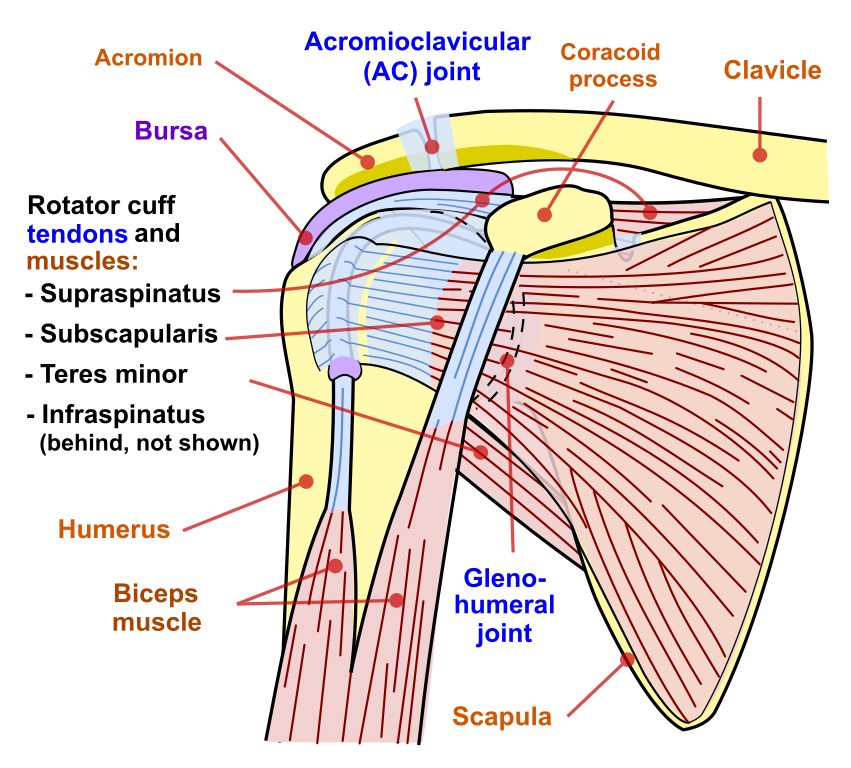
What’s in a Shoulder? Bones and Joints.
The shoulder is a complicated structure comprised of three joints (glenohumeral, acromioclavicular, and sternoclavicular) and one junction (scapulothoracic). There are three main bones to the shoulder (humerus, scapula, and clavicle). But the connections to the axial skeleton via the thoracic cage (scapulothoracic junction and manubrium) should be acknowledged. The glenohumeral joint has six degrees of freedom and is the most mobile joint in the human body. However, the abundant mobility of the shoulder comes with a trade-off. The shoulder has a predisposition to instability and impingement. As a side note, my view is that sub-acromial impingement is a natural state of the shoulder. That is, at the extremes of shoulder abduction or flexion, the sub-acromial structures of the shoulder joint become impinged (i.e., compressed) between the humerus and acromion. Impingement is only a pathological state when the tissue stress exceeds its tolerance (e.g., tissue overload, vascular compromise, inadequate recovery, etc.).
Passive Stuff: Joint Type, Capsule, Ligaments, Labrum



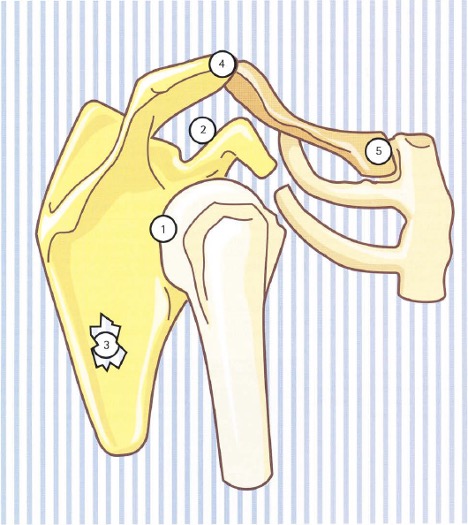
Source: Kapandji, I A. The Physiology of the Joints: Volume 1 The Upper Limb, 2007.
Image 1: (1) Supraglenoid Portion of Superior Band of Glenohumeral Ligament, (2) Coracoid Process, (3) Coraco-humeral Ligament, (4) Supraspinatus, (5) Subscapularis, (6) Tendon of Long Head of Biceps, (8) Tranverse Humeral Ligament, (9) Superior Band of Glenohumeral Ligament, (10) Middle Band of Glenohumeral Ligament, (11) Inferior Band of Glenohumeral Ligament, (12) Foramen of Weitbrecht, (13) Foramen of Rouviere, (14) Long Head of Triceps
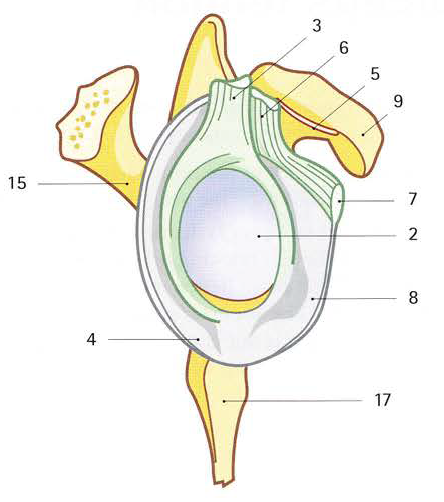
Image 2: (2) Glenoid Cavity, (3) Tendon of Long Head of Biceps (cut), (4) Frenula Capsulae, (5) Subcoracoid Space, (6) Intra-arcticular Portion of Biceps Tendon, (7) Coraco-humeral Ligament, (8) Joint Capsule, (9) Coracoid Process, (15) Root of Spine of Scapula, (17) Inferior Glenoid Tubercle
Image 3: (1) Joint Capsule, (2) Frenula Capsulae, (3) Tendon of Long Head of Biceps (cut), (4) Superior Band of Glenohumeral Ligament, (5) Tendon of Subscapularis (cut)
Image 4: (gl) Glenoid Labrum
The innate instability of the glenohumeral joint arises from the fact that despite being classified as a ball-and-socket joint, the glenoid fossa is very shallow. In addition, the surface area of the humeral head is much larger than the glenoid fossa (in the order of a 4:1 ratio (Chang et al., 2021)). You can think of this as a golf ball on a golf tee. When the ball is directly on the tee, the structure is stable. But it can fall off easily. In the case of the shoulder, that would be a dislocation. However, the passive relative instability of the joint due to its boney configuration, despite being a ball-and-socket structure, is somewhat offset by the capsulolabral complex. The glenoid labrum is a fibrocartilaginous structure that functions as a gasket for the shoulder. It has been hypothesized that the labrum creates a negative pressure within the joint cavity via the surface tension of the synovial fluid between the articular surfaces. Along with the articular cartilage of the glenoid fossa, the labrum also deepens the joint cavity by approximately 50%. While at the same time, the labrum also increases the articular surface area of the glenohumeral joint. Together these factors contribute to the passive stability of the joint.

Furthermore, the limited passive stability afforded to the glenohumeral joint from its osteology is abated by the articular capsule. The ligamentous system of the glenohumeral joint is thickenings of the articular capsule. These ligaments act as primary static stabilizers. Generally, three bands are identified that make up the anterior ligaments of the joint capsule (superior, middle, and inferior). A fourth ligament, the coracohumeral ligament, extends from the coracoid process of the scapula to the humerus and strengthens the superior portion of the articular capsule. For the shoulder to have its substantial range of motion, the ligaments only become tight at the end range of motion. The superior glenohumeral ligament is tight in adduction. The middle glenohumeral ligament is tight at 45 degrees of abduction. And the inferior ligament is taught when the shoulder is abducted to 90 degrees while in lateral rotation. The inferior glenohumeral ligament is considered the strongest and most important passive soft tissue stabilizer (Goetti et al., 2020). The posteroinferior capsule and posterior inferior glenohumeral ligament are not as robust as their anterior counterparts but still contribute to the stability of the joint.
There are also the coracoclavicular ligaments, compromised of two bundles. The trapezoid ligament anteriorly and conoid ligament posteriorly. These ligamentous bundles stabilize the clavicle. As well as the coracoacromial ligament, which helps to protect the head of the humerus. Furthermore, there are ligaments that strengthen the sternoclavicular and acromioclavicular joints as well. The sternoclavicular joint complex is comprised of the following, anterior sternoclavicular ligament, articular capsule, articular disk, costoclavicular ligament, interclavicular ligament, and posterior sternoclavicular ligament. The acromioclavicular joint is comprised of three ligaments (superior acromioclavicular ligament, inferior acromioclavicular ligament, coracoacromial ligament).
For the glenohumeral joint to be centrated (the point at which there is maximum articular surface area contact), tensions anteriorly and posteriorly must be in balance. But joint centration is actively maintained via muscular activation.
The inner lining of the articular capsule is a synovial membrane. This membrane produces synovial fluid to lubricate the articular surfaces. There are also bursae throughout the capsular complex. The bursae are thickened areas of the synovial membrane that secrete synovial fluid and are present where there is increased friction between tissues.
Active Stuff: The Neuromuscular System







Sources: Crompton, Robin Huw, Cummings, Shane W. , Tangen, Christopher and Wood, Bernard. “Human Muscle System”. Encyclopedia Britannica, 5 Nov. 2020, https://www.britannica.com/science/human-muscle-system. Accessed 3 January 2022.
Miniato Muhammad A., Anand Prashanth, Varacallo Mathew. “Anatomy, Shoulder and Upper Limb, Shoulder”. [Updated 2021 Jul 31]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2021 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK536933/
The mobility of the shoulder complex is controlled by 18 muscles that act in synergy. This activity is governed by the nervous system, both at voluntary (somatic nervous system) and involuntary (autonomic nervous system) levels. The nervous system requires a robust amount of proprioceptive information. Proprioceptive information transmits to the nervous system from mechanoreceptors located in the tissue.
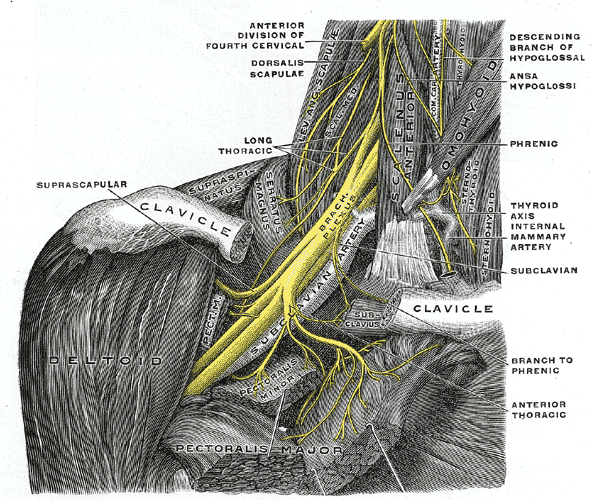

Source: https://en.wikipedia.org/wiki/Brachial_plexus
The innervation of the glenohumeral joint is a function of the suprascapular, lateral pectoral, and axillary nerves. All of the nerves supplying the glenohumeral joint originate from the brachial plexus, a network of nerves formed by the ventral rami of the lower four cervical nerves and the first thoracic nerve (C5, C6, C7, C8, and T1). The cervical and thoracic spine have significant implications for the shoulder complex. But I will omit the details of their roles for this post.

The rotator cuff of the shoulder is integral in maintaining joint centration via the concavity compression mechanism. When muscles contract, they act as a pulley system on the bones they attach to, resulting in angular motion via a moment arm. However, whenever a muscle contracts, it shortens. Hence muscles also compress the articulations that they cross. That is how stability is improved with concavity compression in the glenohumeral joint. However, because muscle attachments have moments to the centre of the axis of a joint, and joint surfaces and orientations vary, muscle contraction also results in translation motion or glide. That is particularly true for the larger, polyarticular muscles that cross the shoulder joint. For the glenohumeral joint to stay centrated, the rotator cuff must work to minimize joint translation, and muscles must work in synergy to develop force couples to maintain joint stability. In my opinion, all the muscles have a role to play as stabilizers depending on the task at hand. Many authors will highlight specific muscles as having more of a stabilizing or mobilizing role. Generally, this role falls on the monoarticular muscles, though exceptions exist, such as the biceps brachii (long head) and triceps brachii (long head).
Movements
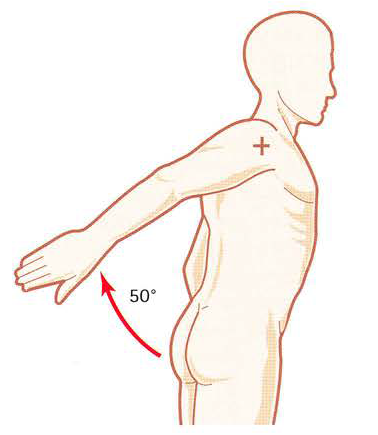

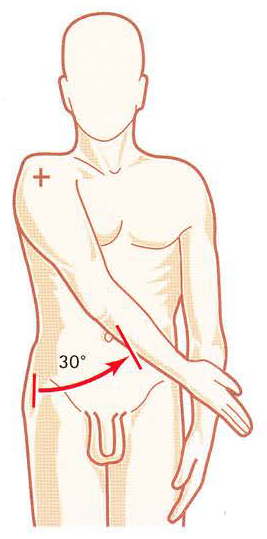
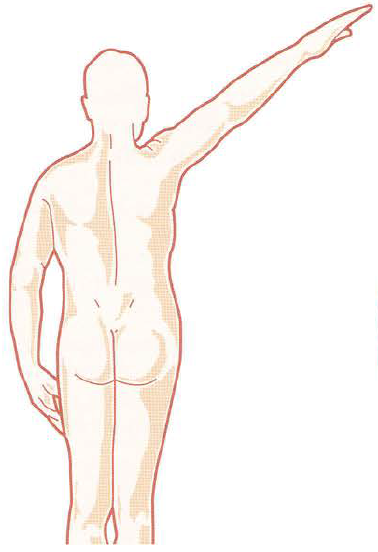

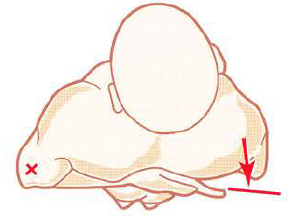
Source: Kapandji, I A. The Physiology of the Joints: Volume 1 The Upper Limb, 2007.
The glenohumeral joint possesses the capability of allowing an extreme range of motion in multiple planes of movement. Flexion, defined as bringing the upper limb anterior in the sagittal plane, has a usual range of motion of 170 to 180 degrees. Flexors of the shoulder include the anterior deltoid, coracobrachialis, and pectoralis major. The biceps brachii also weakly assist in this action. Extension, defined as bringing the upper limb posterior in a sagittal plane, has a normal range of motion of 45 to 60 degrees. Extensors of the shoulder include the posterior deltoid, latissimus dorsi, and teres major. Medial rotation (often referred to as internal rotation), is defined as rotation toward the midline along a vertical axis. The normal medial rotation range of motion is 70 to 90 degrees. Muscles responsible for medial rotation include the subscapularis, pectoralis major, latissimus dorsi, teres major, and the anterior aspect of the deltoid. Lateral rotation (aka. external rotation) is defined as rotation away from the midline along a vertical axis. The normal range of lateral rotation is 90 degrees. Lateral rotation is achieved primarily by the infraspinatus and teres minor. Adduction is defined as bringing the upper limb towards the midline in the coronal plane. The pectoralis major, latissimus dorsi, and teres major are the muscles principally responsible for shoulder adduction. Adduction purely in the coronal plane is only possible to zero degrees. At zero degrees in the coronal plane, adduction is blocked by the trunk. But when combined with slight flexion or extension up to 45 degrees is possible. Abduction is defined as bringing the upper limb away from the midline in the coronal plane. The normal range of motion is 150 to 180 degrees. The movement of abduction is often broken into phases due to the motion arising from both pure glenohumeral abduction and upward rotation of the scapula. Generally, the supraspinatus is responsible for the first 0 to 15 degrees of abduction, the middle fibers of the deltoid are responsible for approximately 15 to 90 degrees, and scapular rotation due to the actions of the trapezius and serratus anterior allow for abduction beyond 90 degrees.
The scapula is also capable of motions. Frequently, six motions are cited (elevation, depression, protraction, retraction, upward rotation, downward rotation). But in addition, the scapulae are also capable of anterior and posterior tilt, as well as medial and lateral rotation (Paine & Voight, 2013). When describing the motions of the scapula the glenoid fossa is used as the point of reference.

The motions of the scapula contribute to the movement of the shoulder complex. The elevation is a superior (cranial) motion of the scapula and is done via the upper trapezius and levator scapulae. The depression of the scapula is in an inferior (caudal) motion. Its done with the lower trapezius and latissimus dorsi. Retraction or adduction is a movement of the scapula toward the midline via the rhomboids and middle trapezius. Protraction or abduction is a movement away from the midline predominantly done by the serratus anterior. Due to the shape of the thoracic cage, both retraction and protraction are coupled movements. During retraction, the scapula moves posteriorly and laterally rotates. And during protraction, the scapula moves anteriorly and medially rotates. Essentially the scapula is following the contours of the thoracic cage by way of the scapulothoracic junction during retraction and protraction. Lateral rotation of the scapula turns the glenoid fossa laterally. And medial rotation turns the glenoid fossa medially. Upward rotation moves the glenoid fossa cranial and medial with contraction of the upper and lower trapezius and serratus anterior muscles primarily. And downward rotation moves the glenoid fossa caudal and lateral by way of the rhomboids, levator scapulae, and pectoralis minor. The scapula anteriorly tilts by turning a transverse axis bringing the glenoid fossa anteriorly. The glenoid fossa moves posteriorly when the scapula posteriorly tilts. The motions are controlled predominantly via a force couple between the pectoralis minor and serratus anterior.
Both the mobility and stability of the scapula are paramount to the overall function of the shoulder. If the scapula is immobile, then there is a greater risk of developing impingement conditions due to the abutment of the humerus into structures like the acromion or coracoid process. At the same time, the overall mobility (and stability) of the shoulder complex will be limited due to altered scapulohumeral kinematics. The scapula must also be stable to facilitate a base of support for the humerus to generate force.
The Plumbing: Vasculature and Lymphatics
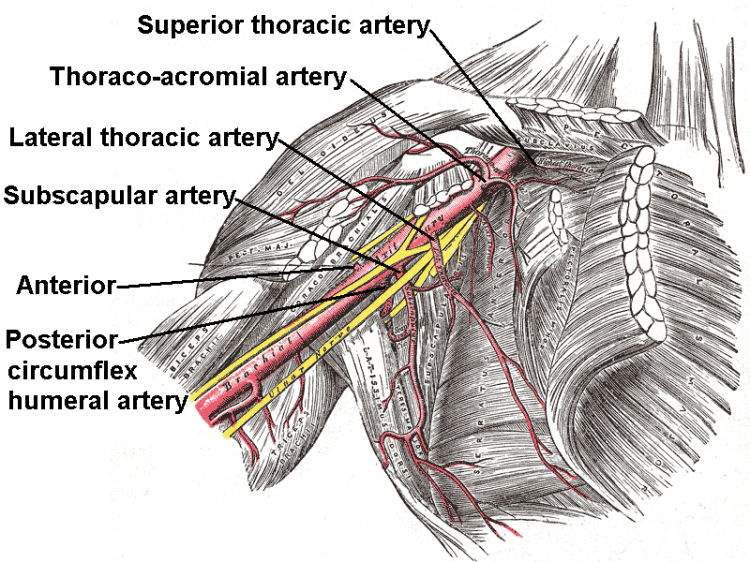
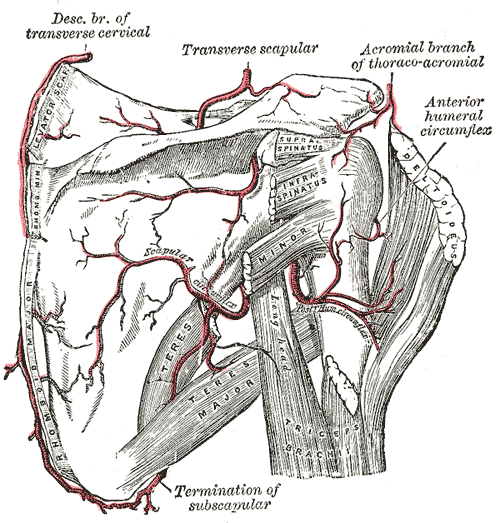
Source: https://en.wikipedia.org/wiki/Anterior_humeral_circumflex_artery
The glenohumeral joint receives vascular supply via the posterior and anterior circumflex humeral arteries, both of which are branches of the axillary artery. The predominant arterial blood supply to the humeral head is via the posterior humeral circumflex artery. But there are anastomoses with other vessels.

The majority of the lymph nodes in the upper extremity are located within the axilla. These can be divided based on their location into five main groups: pectoral, subscapular, humeral, central, and apical. Efferent vessels coming from the apical axillary nodes travel through the cervico-axillary canal and then converge to form the subclavian lymphatic trunk. This trunk will either continue to enter the right venous angle or drain directly into the thoracic duct on the right and left, respectively.
The vascular and lymphatics systems of the body are important for both performance and regeneration. However, generally, they are viewed from a medical pathoanatomical perspective.
Wow! That was a lot. Stayed tuned for Volume 2 where I might actually get into some SUP-specific shoulder mechanics…

{kind=link}
{kind=link}
3 thoughts on “SUP Biomechanics: Shoulders Volume 1”