
Anatomy 103
Saturday, October 22, 12022 HE
A word of warning. My interest in anatomy started in high school when I got into strength training. Anatomy was then my favourite subject during my undergraduate degree in Human Kinetics. It remained my favourite subject during my Physical Therapy studies. It was still my favourite topic when I completed a Diploma in Manual Osteopathy. All this is to say that this may go into too much detail for the less anatomically enthused. If you are keener on the application to Stand Up Paddleboarding (SUP), skip ahead a post to “Lower Back: Volume 2” of this installation.
Full disclosure, I am a licensed physical therapist and manual osteopathic practitioner, but the following is purely for informational purposes. For formal guidance concerning your stand up paddleboard (SUP) biomechanics, it may be in your interests to seek out the aid of a licensed/qualified professional. If you are experiencing pain with physical activity, exercise a degree of caution when evaluating the nature of your symptoms. Pain with movement or exertion can be a normal symptom, but it may also signal something more nefarious. Use your own personal judgement, but if in doubt, err on the side of caution for a proper evaluation licensed/qualified medical professional.
- Anatomy 103
- Biomechanical Overview
- Mobility and Stability Subsystems
- Structure and Function
- Passive Stuff: Bones, Capsules, and Ligaments
- Active Stuff: The Neuromuscular System
- What About the Guts?
- Movements
- Lumbar Plumbing: Vasculature and Lymphatics
Biomechanical Overview
This post is my sixth on SUP biomechanics. The first post was a general overview of SUP biomechanics, which you can see here. For the second one, on shoulder anatomy, click here. For the third, on SUP stroke shoulder biomechanics, click here. For the fourth post on hip anatomy, click here. For the fifth, on SUP stroke hip biomechanics, click here. This post will cover the pertinent anatomy of the lower back for SUP. Anatomy, like many subjects, is easier to learn when reduced to its constituent parts. But at a functional level, anatomy is much more complex and interrelated. The lower back or its parts do not function in isolation or independently. Anatomy is regionally interdependent. Anatomy and physiology are more of an emergent phenomenon, where the whole is greater than the sum of its parts.
Stand up paddleboarding is a quickly growing aquatic recreational and sporting activity. It is easily accessible to most people since it requires minimal equipment and is easy to learn. It can be practiced on almost any body of water and provides a low-impact, full-body physical challenge suitable for all ages and skill levels. As with any activity, SUP has risks (see this post for general SUP safety guidelines). Concerning musculoskeletal injuries, a 2017 study by Furness and colleagues revealed that the shoulder/upper arm was the most frequently injured body location (32.9% of all injuries). Hence why my first posts on SUP biomechanics focused on the upper extremity. In the study by Furness and colleagues, the lower back was the second most commonly reported injury site, at 14.3% of all injuries. The hip/buttock only accounted for 3.7% of all injuries reported. But as explained in my hip posts, Volume 1 and Volume 2, the hips’ relationship to the lower back is significant. Readers may be familiar with the idea that back pain is commonplace. In developed nations, the lifetime incidence of reported lower back pain is between 75-84%. You are likely to have back pain at some point in your life. However, globally the incidence of lower back pain is overall low (i.e., <1%), with a prevalence of around ~8% (15th worldwide cause), and is responsible for 2.6% of all disability-adjusted life years (DALYs; 6th worldwide cause of DALYs). So the effects of low back pain on society are significant. Regular physical activity is one contributor to reducing the burden of disease. Therefore, it is preposterous to partake in SUP as physical activity and risk lower back pain with preventably poor practices. The adage of the seven P’s comes to mind: proper planning and practice prevent piss-poor performance.
Schram and colleagues’ 2019 paper compared the stroke biomechanics of experienced and inexperienced paddlers. The study’s main finding was that experienced paddlers used less shoulder movement and more hip movement. The data was collected on a KayakPro SUP ergometer, and did not look at injuries specifically. It only compared the biomechanics between the two groups. You can see animations of two representative paddlers (one experienced, one inexperienced) created from their data in the video clip below.
Hip vs. Back
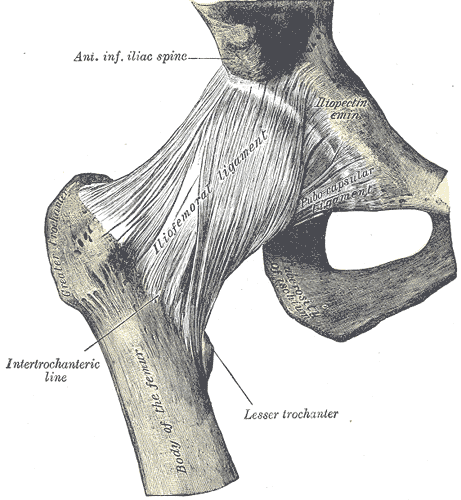
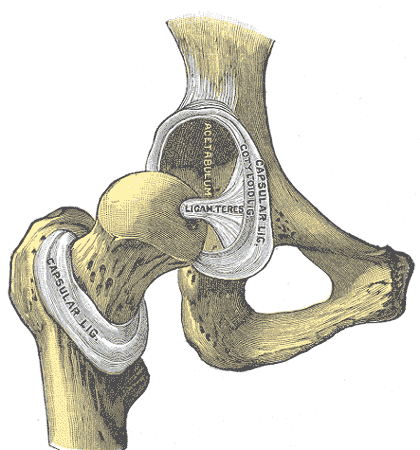
The experienced paddler on the left demonstrates much more full-body movement than the inexperienced paddler on the right. Note how much more the experienced paddler’s pelvis and therefore, hips move. Also, notice the difference in how the ribcages of both paddlers move through space. The experienced paddler’s torso exhibits much more global motion, specifically rotation, in the transverse plane about a longitudinal (aka., cephalocaudal) axis. Much of the movement of the ribcage results from the movement of the hips and pelvis below. As stated in my hip post, the hip joint is a diarthrosis, a ball-and-socket synovial joint ideal for motion and stability.


Types of Joints: Schematic

Source: https://openstax.org/books/anatomy-and-physiology-2e/pages/9-4-synovial-joints
Back vs. Hip
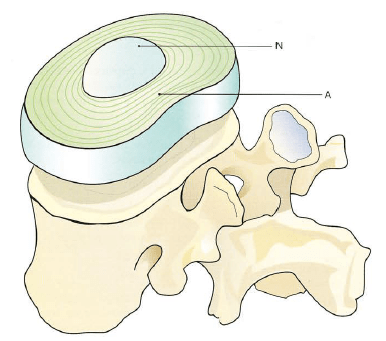
Whereas, the intervertebral joints are a three-joint complex, the articular triad. There is one amphiarthrosis joint between the vertebrae, a fibrocartilaginous joint that allows for movement but is not ideal for large-scale repetitive motion. And a pair of synovial joints between the facets of adjoining vertebral arches (i.e., zygapophyseal joints or facet joints). The term “zygapophyseal” is derived from the Greek words “physis”, meaning outgrowth, and “zygos”, meaning yoke or bridge. Therefore, the original meaning of “zygapophyseal” is “bridging of outgrowths” (Inoue et al., 2019). The complex is capable of motion, but as will be discussed, too much motion can result in discogenic pathology. Readers will likely be familiar with the term “slipped disc” (or a herniated disc), and we will discuss its etiology below and how optimal biomechanics can reduce the risk of disc injury.




Sources: https://commons.wikimedia.org/wiki/Gray%27s_Anatomy_plates#/media/File:Gray92.png
Kapandji, I A. The Physiology of the Joints: Volume 3 The Spinal Column, Pelvic Girdle and Head, 2008.
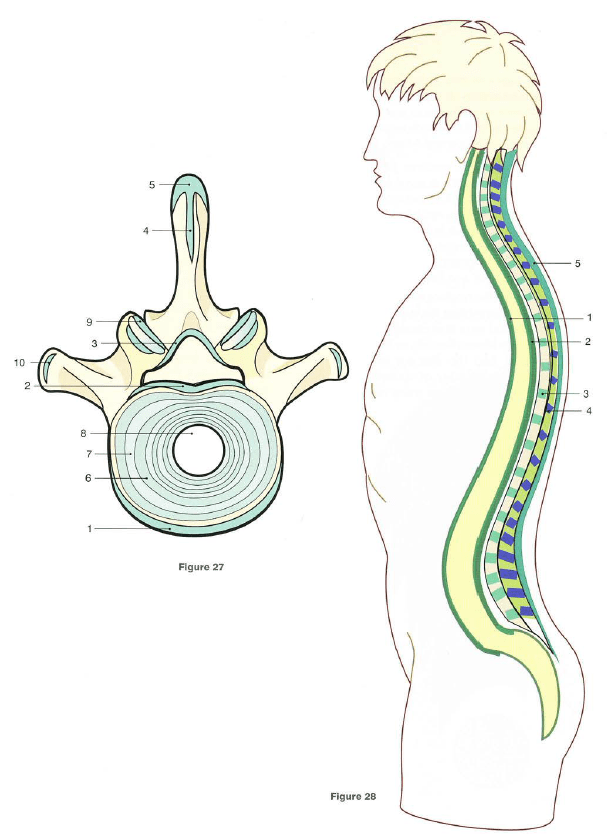
Image 4: (1) anterior longitudinal ligament, (2) posterior longitudinal ligament, (3) ligamentum flavum, (4) interspinous ligament, (5) supraspinous ligament, (6 and 7) concentric layers of the annulus fibrosus, (8) nucleus pulposus, (9) anterior and posterior ligaments of the zygapophyseal joint capsule, (10) intertransverse ligament
Image 5: (N) nucleus pulposus, (A) annulus fibrosus
As I did for the shoulder and hip posts, I would like to cover some lumbar spine anatomy before delving into the biomechanics (for more details, see Sassack and Carrier, 2021; Miele et al., 2012; Inoue et al., 2019). You can use Sci-Hub to access the full text of the articles if you do not have access via another means.
Mobility and Stability Subsystems
Again, Panjabi’s (1992) landmark theoretical model for spinal stability is a great framework to conceptualize the stability of the joint structure. The model was originally developed for spinal stability. Simply, he proposes that three subsystems (neural, passive, and active) govern the overall biomechanical control of a joint. Below is a schematic of Panjabi’s model and an expanded version by Hoffman and Gabel (2013) highlighting the expression of movement (i.e., mobility and stability). This model applies to all the articulations in the body. As was the case for the shoulder and hip, for the lumbar spine to be stable and functional, there must be cooperation between the various subsystems contributing to mobility and stability.

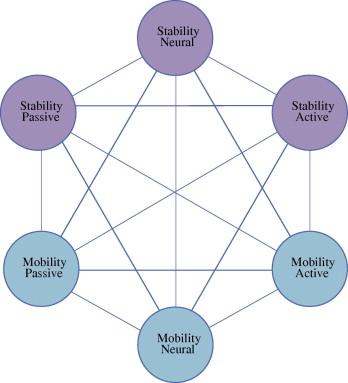
Source: Hoffman, J., and P. Gabel. “Expanding Panjabi’s Stability Model to Express Movement: A Theoretical Model.” Medical Hypotheses, vol. 80, no. 6, 2013, pp. 692–697., https://doi.org/10.1016/j.mehy.2013.02.006.
Structure and Function
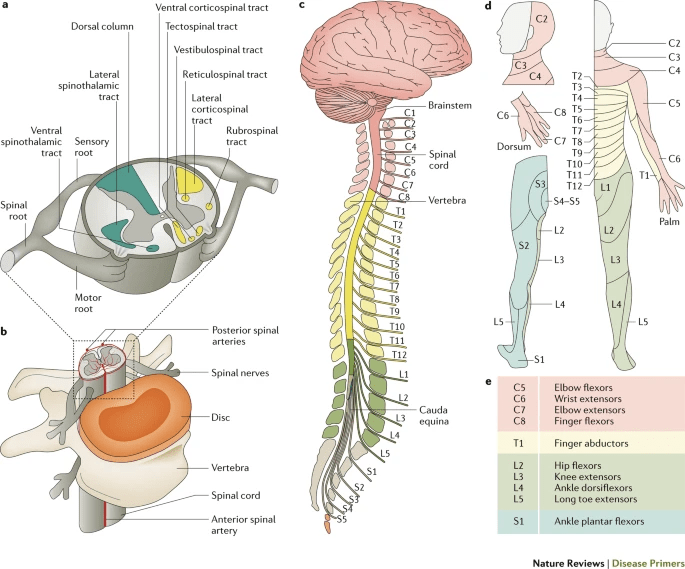
Three main functions of the lumbar spine are commonly cited, support, protection, and motion. First, the lumbar spine assists in supporting the upper body. The lumbar vertebrae are larger compared to other regions of the spine. Their sheer size allows them to absorb axial forces delivered by the structures above, i.e., the head, neck, and trunk. The second function is protection. The spinal canal is the hole that runs down through all your vertebral segments and houses the spinal cord. The vertebrae thus protect the spinal cord and spinal nerves. Therefore, the health and function of the lumbar spine are integral in the communication of the central nervous system to the lower extremities. Third, the lumbar spine allows for diverse types of truncal motion, which will be covered in more detail below. The spine enables both neurological and biomechanical communication between the upper and lower body segments allowing for ambulation and locomotion.
What’s in a Lower Back?
Important Cargo
The spinal cord is a soft, pliable mass of nerve fibres and cells supported by glial tissue. The spinal cord runs the course of the spinal column from the bottom of the brain stem (i.e., the medulla oblongata) to where it tapers around the L1/L2 vertebral level, the conus medullaris. The spinal cord (and brain) is protected by three layers of tissue or membranes, called meninges, surrounding the canal. The outermost layer is the dura mater is a tough protective coating. In between the dura mater and the surrounding vertebral bone is the epidural space filled with adipose tissue and a network of blood vessels. The arachnoid mater is the middle layer named for its open spiderweb-like appearance. The space between the arachnoid mater and the underlying pia mater is called the subarachnoid space and is filled with cerebrospinal fluid. The delicate innermost protective layer, the pia mater, is tightly associated with the surface of the spinal cord. The spinal cord is stabilized within the dura mater by the connecting denticulate ligaments, extending from the enveloping pia mater laterally between the dorsal and ventral roots. The dural sac ends at the vertebral level of the second sacral vertebra. The dura mater covering the spinal cord is firmly attached to the base of the skull and the second fused segment of the sacrum in the adult via the filum terminale.
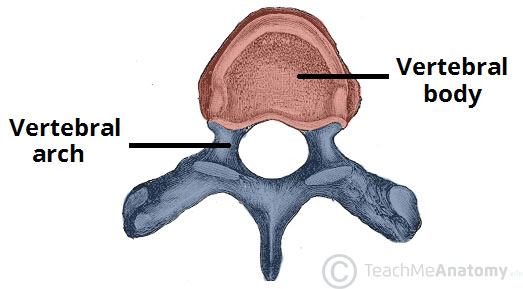
Anatomy of a Vertebrae
Typically, the lumbar spine in humans is comprised of five segments. They are numbered from top to bottom as L1 to L5. The entire spine is made up of 33 pieces. From top to bottom, the spine can be partitioned into three mobile (seven cervical, 12 thoracic, and five lumbar) and two fused regions (five sacral, and four coccygeal). Each lumbar vertebra consists of multiple components. A vertebra can be divided in half into its ventral (or anterior) structure, the vertebral body, and its dorsal (or posterior) structure, the vertebral (or neural) arch. The vertebral body is the main load-bearing structure of the spine (Miele et al., 2012). It is primarily composed of cancellous (or trabecular/spongy) bone encased in an outer shell of cortical (or compact) bone. Cancellous bone is an anisotropic viscoelastic material. Thus, it is able to deform and absorb force. In fact, one view on spinal stability suggested by Stuart McGill is that the properties of the trabecular bone of vertebrae, along with the valveless vertebral venous plexus (aka., Batson plexus), may act as the main shock absorption mechanism of the spine. This view contrasts the commonly suggested role of the intervertebral disc as the primary shock absorber. To me, the trabecular hypothesis makes more sense given the relative incompressibility of the nucleus pulposus, given it is a gelatinous substance.
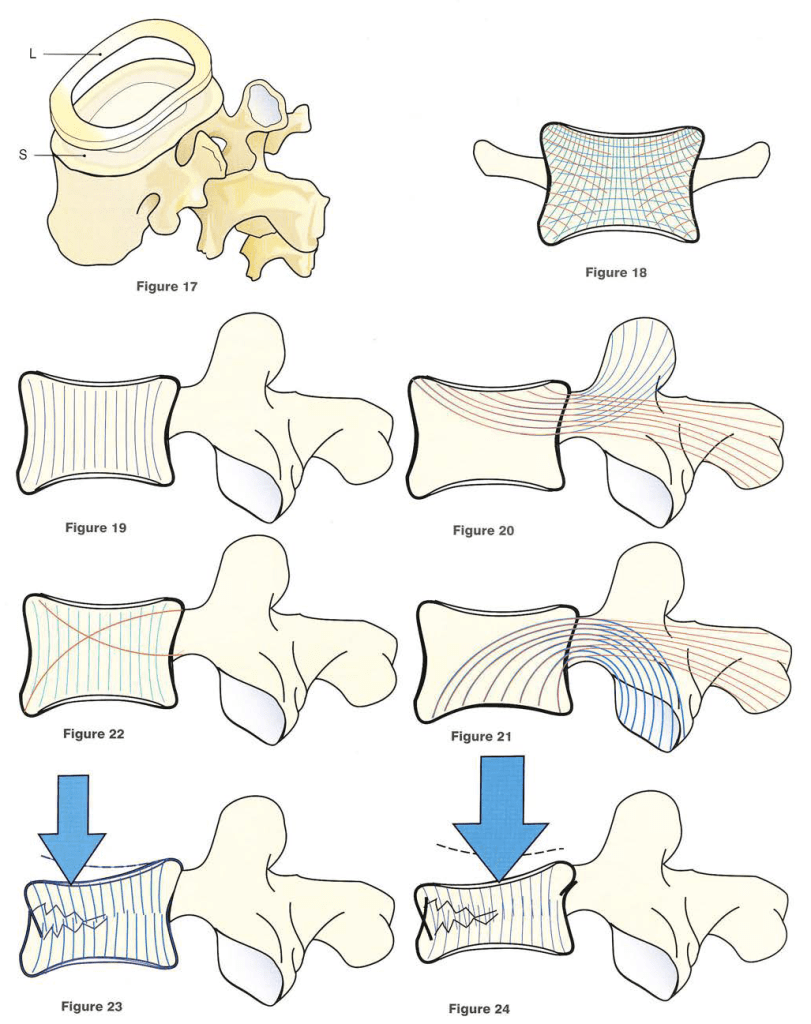
Source: Kapandji, I A. The Physiology of the Joints: Volume 3 The Spinal Column, Pelvic Girdle and Head, 2008.
Figure 17: (L) labrum, (S) discal surface
Thus, conceptually the vertebral column can be seen as two distinct columns, a ventral and dorsal column, connected by bridges creating the space for the spinal canal (Miele et al. 2012). The bridges to the posterior elements of the vertebral arch are pedicles that attach to the laminae. The arches created by a superior and inferior pair of pedicles create the intervertebral foramen. A number of structures pass through the foramen, the most important of which is the spinal nerve root. The pedicles resist motion and transmit forces from the posterior elements to the vertebral body. The two laminae meet, forming the spinous process extending posteriorly. At the junction between the pedicles and laminae, four articular processes reside, a superior and an inferior pair. Protruding laterally, are two transverse processes, one on each side of the vertebrae. The laminae, transverse processes, and spinous processes serve as attachment points for ligaments and musculature. The superior and inferior articular processes create the zygapophyseal joints.
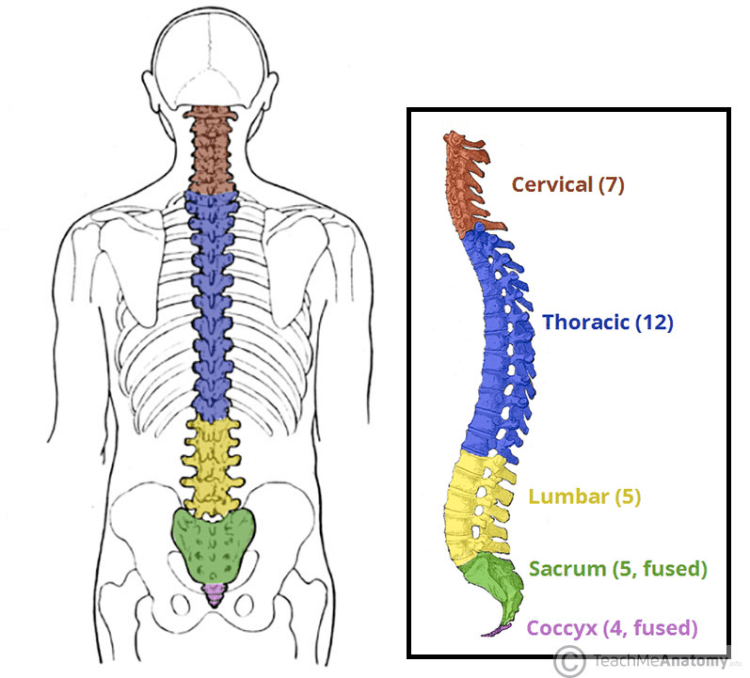
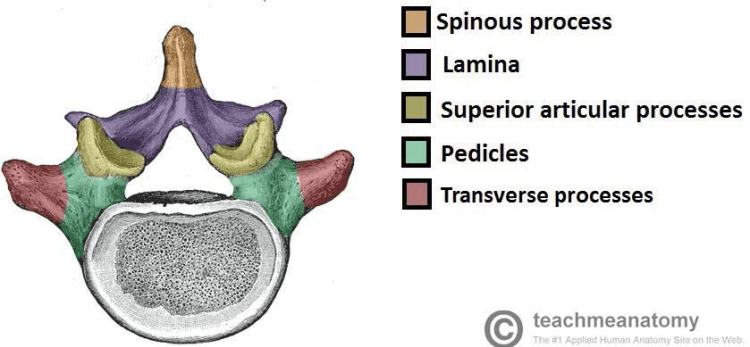
Source: https://teachmeanatomy.info/back/bones/vertebral-column/
Linking it Together: Joints
As mentioned, the vertebral segments of your lower back are an articular triad, with three joints for each pair of bones. The lumbar intervertebral disc serves as a fibrocartilaginous joint connecting the vertebral endplates of two adjacent segments. Each vertebra has a pair of ‘facets’ on either side of the vertebral column. The term “facet” is a bit of a misnomer as they are not actually flat structures (Inoue et al., 2019). The superior facets of inferior vertebrae combine with the inferior facets of the vertebrae immediately cephalad to form the synovial zygapophyseal joints. In the lumbar spine, the zygapophyseal joints lie in the sagittal plane, which facilitates the motion of flexion and extension in the lumbar spine. The pars interarticularis is the location of the lamina between the superior and inferior articular processes. It is an area prone to develop stress fractures (spondylolysis) in the growing spine, with an estimated occurrence in one out of 20 people.
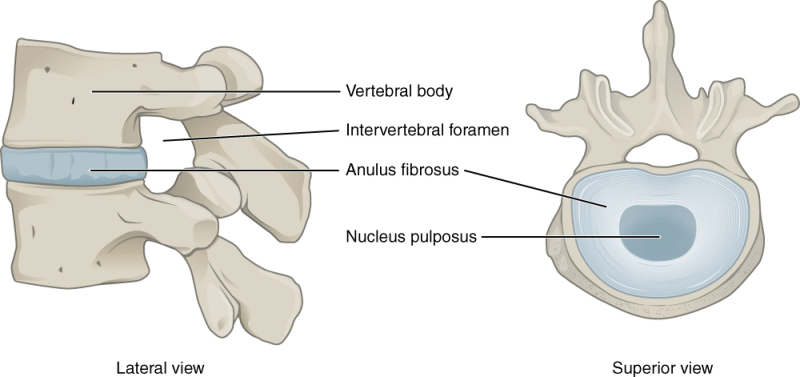
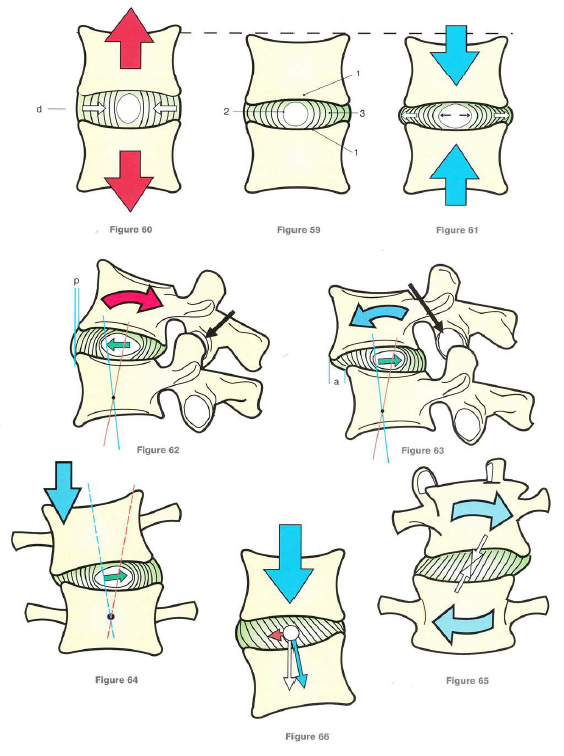
The intervertebral disc is comprised of an internal gelatinous nucleus pulposus and external fibrous annulus fibrosus. The nucleus pulposus is essential for the mechanical flexibility and strength of the spine. Comprised of water, type II collagen, chondrocyte-like cells, and proteoglycans (sulfated glycosaminoglycans), the nucleus pulposus has elastic properties, making it flexible under stress and compression resistant. It is located posterocentral (the image below does not reflect this) in the intervertebral disc and makes up 30-50% of the cross-sectional area (Miele et al., 2012).
The annulus fibrosus serves to contain the gelatinous nucleus pulposus. It is composed of concentric layers of collagen fiber bundles wound in a helicoid manner. The layers are type I collagen fibers, which alternate in alignment, with adjacent layers at approximately 120-degree angles from one another. The layered collagen orientation allows for greater resistance to shearing and rotational forces (Miele et al. 2012). I will touch on this again later with the biomechanics. The design also allows for equal distribution of forces from concentric axial loads. With eccentric loads, the nucleus will migrate to the opposite side of the imposed stress and bulge at the annulus fibrosis. If the stress tolerance of the annulus is surpassed a pathological condition of disc herniation can occur. Often this can be considered a sequentially staged process, occurring over time, though rarely a single traumatic event could cause the damage. Typically, a herniation results from repetitive flexion with higher loads on the spine. This process delaminates the collagen fibres, allowing the nucleus pulposus to work through the layers of the lamina, eventually creating a bulge. It is the proverbial straw that broke the camel’s back. It is not the straw, rather it is the multitude of straws beneath it. When you herniate a disc, it is not one specific event in question, it is a build-up of behaviours that is the cause.
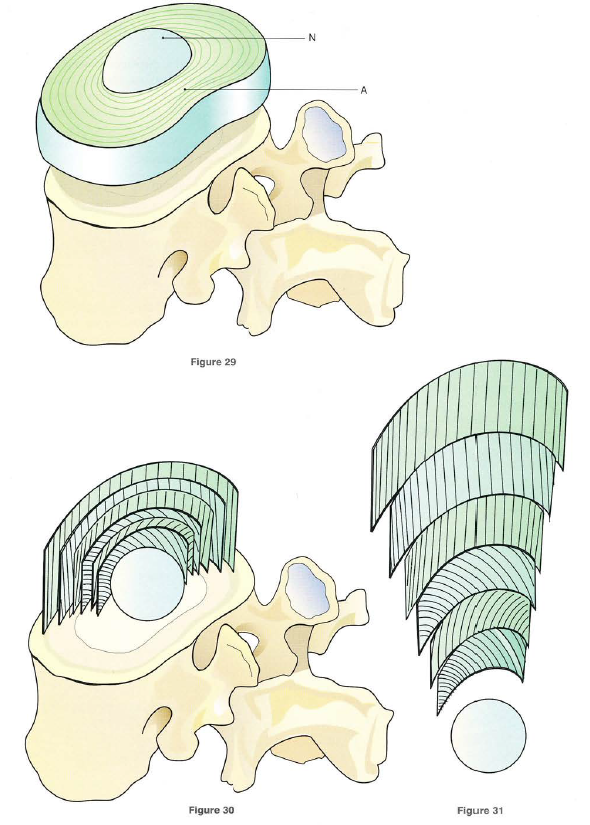
Source: Kapandji, I A. The Physiology of the Joints: Volume 3 The Spinal Column, Pelvic Girdle and Head, 2008.
Figure 29: (N) nucleus pulposus, (A) annulus fibrosus
Transitions
The lumbar spine is part of the axial skeleton and is situated between the thoracic spine and sacrum. In fact, the lumbar spine can be seen as part of a larger subunit of the body, the lumbopelvic-hip complex. The body is a regionally interdependent system, and as such, the form and function of adjacent structures have effects. Via the lumbosacral and sacroiliac joints, the lumbar spine is connected to the pelvic girdle and thus the appendicular skeleton. The inferior articular processes of the L5 vertebrae are orientated in the coronal (frontal) plane to articulate with the S1 segment. The transition alters the motion available but also serves as a mechanical restraint to prevent anterior translation of the spinal column on the sacrum. Similarly, the superior articular processes of the L1 vertebra change orientation to be more aligned in the coronal plane. This change affords the thoracic spine more movement in the coronal plane. It is worth noting the changes in the architecture of the spine coincide with the change in functional curvature from a lordosis to kyphosis. The transition areas of the spine are more susceptible to injury degenerative changes due to abrupt changes in “stiffness” at these junctions (Miele et al. 2012).

(1) sacral curvature, (2) lumbar curvature (aka. lordosis), (3) thoracic curvature (aka. kyphosis), (4) cervical curvature (aka. lordosis)
Passive Stuff: Bones, Capsules, and Ligaments
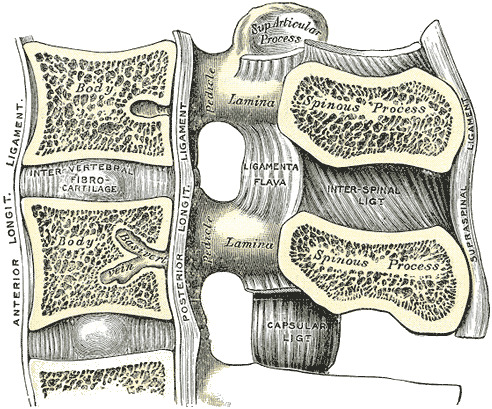
Source: Kapandji, I A. The Physiology of the Joints: Volume 3 The Spinal Column, Pelvic Girdle and Head, 2008.
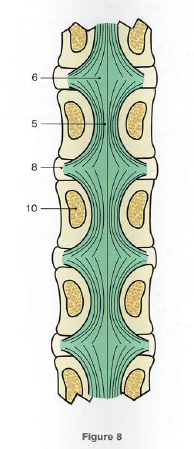
(1) Anterior Longitudinal Ligament, (2) Posterior Longitudinal Ligament, (3) Ligamentum Flavum, (4) Interspinous Ligament, (5) Surpaspinous Ligament, (6-7) concentric layers of the Annulus Fibrosus, (8) Nucleus Pulposus, (9) Anterior and Posterior Ligaments of the Zygapophyseal Joint Capsule, (10) Intertransverse Ligament
Part of the inherent stability of the lumbar spine arises from its osteology (i.e., its structure). The size of the vertebral body, as well as, the size and orientation of the articular and spinous processes and zygapophyseal joints, provide an innate degree of mobility and stability. The sagittally aligned zygapophyseal joints and more horizontally orientated spinous processes promote more flexion and extension. The zygapophyseal joint acts as a check to axial rotation and probably, to a lesser degree, lateral bending. While the shorter, more horizontal spinous processes allow for more extension in the lumbar spine, particularly compared to the anatomy of the thoracic spine.
As mentioned before, adjacent vertebrae are connected via an articular triad. The intervertebral disc is encapsulated by the laminar structure of the annulus fibrosus. The annulus fibrosus can be conceptualized as a ligament as it is a fibrous structure connecting two bones. Meanwhile, as true synovial joints, the zygapophyseal joints are surrounded by a capsule. The joint capsule has thickenings described by various authors but named differently (e.g., “transverse strengthening ligaments” by Putz (1985), “anterior and posterior ligaments” by Kapandji (2008), and “capsular ligaments” by Miele et al. (2012)). These ligaments help to reinforce the joint capsule and limit excess ranges of motion.

[1], superior articular process; [2], inferior
articular process; [3], ‘transverse ligaments’ of the joint capsule; [4], interspinous ligament.
Two longitudinal ligaments lie anterior and posterior to the vertebral body and run the course of the spine. The anterior longitudinal ligament runs down the ventral surface of the spinal column. The anterior longitudinal ligament resists lumbar extension, translation, and rotation. The anterior longitudinal ligament is thick and slightly more narrow over the vertebral bodies and thinner but marginally wider over the intervertebral discs. The posterior longitudinal ligament runs down the dorsal surface of the anterior column, that is, the dorsal surface of the vertebral body and the anterior margin of the spinal canal. The posterior longitudinal ligament resists lumbar flexion. It also helps to reinforce the intervertebral disc against herniation. This reinforcement is crucial since a posterior herniation has the potential to compress the spinal cord. Fortunately, many herniations occur centrally where the space in the spinal canal is large enough to avoid compressing the cord. The posterior longitudinal ligament runs through the spinal canal. The posterior longitudinal ligament narrows at vertebral bodies to accommodate the pedicles and covers the basivertebral veins. It widens at the intervertebral disc space. Despite widening, lumbar intervertebral discs are susceptible to posterolateral herniation which can compromise the neurological structures in the intervertebral foramen and lead to radiculopathy.

Source: Kapandji, I A. The Physiology of the Joints: Volume 3 The Spinal Column, Pelvic Girdle and Head, 2008.
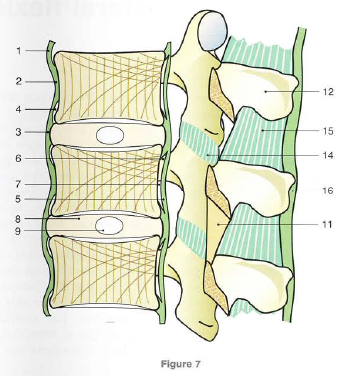
1: Anterior Longitudinal Ligament, 2: Anterior Surface for Vertebral Body, 3: Anterior Aspect of Intervertebral Disc, 4: Potential Space for Osteophyte Formation in Spinal Osteoarthritis, 5: Posterior Longitudinal Ligament, 6: Arcuate Fibres of Posterior Longitudinal Ligament 7: Space for Paravertebral Venous Plexus, 8: Annulus Fibrosus 9: Nucleus Pulposus, 10: Pedicle, 11: Ligamentum Flavum, 12: Spinous Process, 13: Vertebral Canal (posteriorly), 14: Ligaments of the Zygapophyseal Joint Capsule, 15: Interspinous Ligament, 16: Surpaspinous Ligament, 17: Intertransverse Ligament
The third multisegmental spinal ligament is the supraspinous ligament. The supraspinous ligament originates as the ligamentum nuchae of the neck and extends the length of the spine, attaching firmly to the tip of each spinous process. The supraspinous ligament is posterior to the interspinous ligament but is continuous with this segmental ligamentous structure. The supraspinous ligament limits flexion. The interspinous ligaments connect adjoining spinous processes and serve to limit flexion. The intertransverse ligaments run between adjacent transverse processes and often blend with the intertransversarii muscles. The function of the intertransverse ligaments is to limit lateral flexion of the spine. The ligamenta flava (singular, ligamentum flavum, Latin for yellow ligament) connects the laminae of adjacent vertebrae. The yellow colour of the ligamentum flavum arises from its higher elastin content compared to other ligaments. This marked elasticity of the ligamentum flavum serves to preserve an upright posture, and assist the vertebral column in returning to an upright posture after flexion. The elastin helps to prevent buckling of the ligament into the spinal canal during extension, which would compress the spinal cord.

Sources: https://www.ncbi.nlm.nih.gov/books/NBK557616/
https://learnmuscles.com/blog/2017/08/30/ligaments-of-the-lumbar-spine-and-pelvis
Active Stuff: The Neuromuscular System


Source: https://commons.wikimedia.org/wiki/Gray%27s_Anatomy_plates
The nervous system ultimately controls the mobility of the lumbopelvic-hip complex. A friend recently sent me some clips of Lex Fridman‘s podcast interview with Michael Levin. The clips were absolutely fascinating (on how to cure cancer and an explanation of bioelectricity). They left me wanting to listen to the entire episode, “Biology, Life, Aliens, Evolution, and Xenobots,” where Levin made profound insights and challenges to our current conception of biology and the mechanism of evolution. I found Levin’s perspective that “evolution doesn’t produce specific solutions to specific environmental problems. It produces problem solving machines,” absolutely fascinating. I am now envisioning the human nervous system through this perspective. The nervous system is a coordinated stimulus and response system that via evolution and phylogenesis, emerged from complex cellular networks to facilitate organismal-level behaviours. A key adaptation was the development of motor control to better interact with space. Today we are left with a more voluntary (the somatic nervous system) and involuntary (the autonomic nervous system). We distinguish between the two systems, but the dichotomy is denominal, not necessarily biological. The body system requires a coordinated response from all aspects of the nervous system to function. Motor control of the nervous system requires a robust amount of proprioceptive information. Proprioceptive information transmits to the nervous system from mechanoreceptors located in the tissue. The mechanoreceptors are specialized sensors in the tissues that respond to compression or distraction as part of the stimulus-response interaction that drives behaviour.
Lower Back Wiring
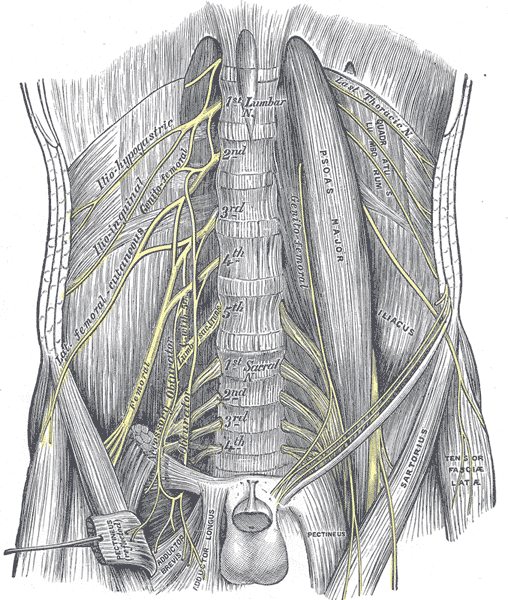
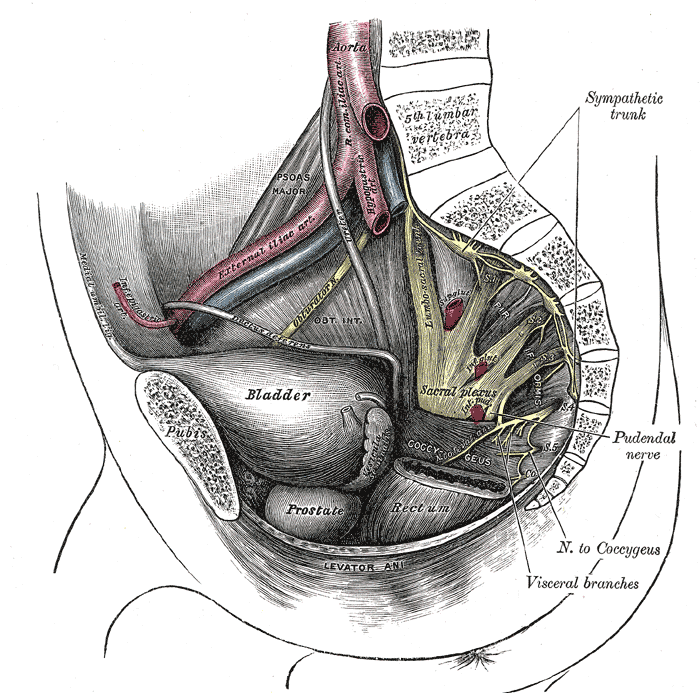
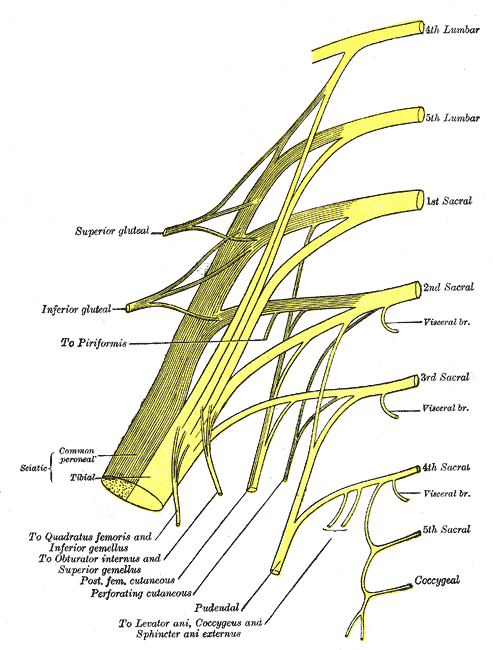
With respect to motor control there are five pairs of mixed spinal nerves emerge from either side of the lumbar spinal cord. Mixed spinal nerves carry both efferent (motor) and afferent (sensory) nerve fibers. The T12 to L4 ventral rami combine to form a network of nerves called the lumbar plexus. The lumbar plexus gives rise to six major nerve branches, the iliohypogastric (T12-L1), ilioinguinal (L1), genitofemoral (L1-L2), lateral cutaneous femoral (L2-L3), obturator (L2-L4), and femoral (L2-L4). There are also short branches that go directly to the muscles of the psoas major (L1-L3), quadratus lumborum (T12-L4), and lumbar intertransverse (T12-L4) nerves. The L4 and L5 nerve roots join to form the lumbosacral trunk, which descends into the pelvis joining the sacral plexus. Together the lumbar and sacral plexus, along with the pudendal plexus, form the lumbosacral plexus. The lumbosacral plexus gives rise to these nerves, the superior gluteal (L4-S1), inferior gluteal (L5-S2), posterior cutaneous femoral (S1-S3), perforating cutaneous (S2-S3), sciatic (L4-S3), pudendal (S1/2-S4), and coccygeal (S5-Co1) nerves. The lumbar nerves are generally responsible for the motor and sensory function of the lower extremity. Though superior nerves from the lumbar plexus also contribute to the lower abdomen and pelvis. For more on these nerves, where they go, and what they innervate, click the links above or check out these tables: “Nerves of the lumbar plexus” and “Nerves of the sacral plexus.” Keep in mind that each lumbar spinal nerve exits below its corresponding vertebra. For example, the L4 nerve exits below the L4 vertebra through the L4-L5 neural foramen. Suffice it to say that it is complicated.

Source: https://commons.wikimedia.org/wiki/Gray%27s_Anatomy_plates
Complicating things more, and possibly more relevant, is that the innervation for the muscles responsible for the motor control of the lumbar spine mostly originates at the thoracic level. Regional interdependence rears its head once again. The major nerves to the anterolateral abdominal wall include the thoracoabdominal (T7-T11), intercostal nerves (T1-T11), subcostal (T12), iliohypogastric (T12-L1), and ilioinguinal (L1) nerves. Therefore, the biomechanics of the upper torso can affect the lower back and abdomen.
A Quick Clinical Note
Each spinal nerve will supply a general area of skin with afferent sensory fibers. The skin area is known as a dermatome. Each spinal nerve also innervates a group of muscles with motor fibers, known as a myotome. Dermatomes and myotomes trace back to our embryological development and are a subdivision of a somite. Dermatomes and myotomes are clinically useful in determining the lumbar spinal nerve(s) pathology. There are even boney tissue groups that are innervated by specific spinal segments called sclerotomes. It gets more complicated when considering the clinical concepts of referred and radicular pain, which I touched on here in my “Hips Volume 1” post. For more information on dermatomes and myotomes, see this section of “Anatomy, Back, Lumbar Spine” (Sassack & Carrier 2022).
Sinew, Might, and Brawn
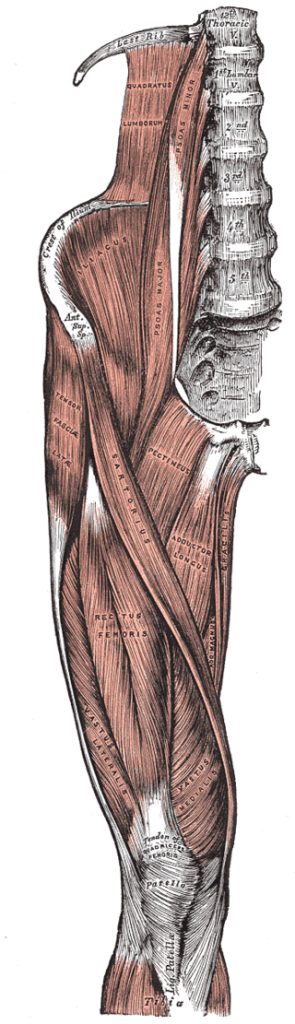
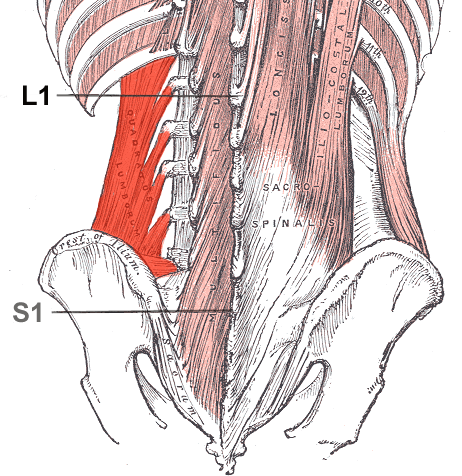
Many muscles attach to the lumbar vertebrae. The muscles allow for controlled, coordinated movement and play a role in stabilization, proprioception, and protection. Three major muscle groups are often identified that originate or insert on the lumbar spine and aid movement. The extensor group consists of the erector spinae and the transversospinales group. In the lumbar region, the erector spinae muscles include the longissimus thoracis and iliocostalis lumborum. The lumbar transversospinales group consists of the multifidi and rotatores lumborum. These muscles are rich in mechanoreceptors and play an intricate role in proprioception. Collectively this group creates an extension moment at the lumbar spine. The lumbar flexor attached directly to the spine is the psoas major. The psoas major originates from the T12-L4 vertebral bodies of T12-L4, intervertebral discs between T12-L4, and transverse processes of L1-L5. The psoas major joins the iliacus muscle to insert onto the thigh at the lesser trochanter as the iliopsoas (composite) muscle. Slightly less than two-thirds of the population has an additional muscle, the psoas minor. The psoas minor is located in front of the psoas major, originating from the last thoracic and the first lumbar vertebra. Distally, it converges with the iliac fascia and the psoas major tendon to insert into the iliopectineal eminence. The psoas major lies anterior to the lumbar spine and allows for trunk flexion, as well as, hip flexion. The iliopsoas’ role is hip flexion. It also assists with the arching of the lumbar spine.
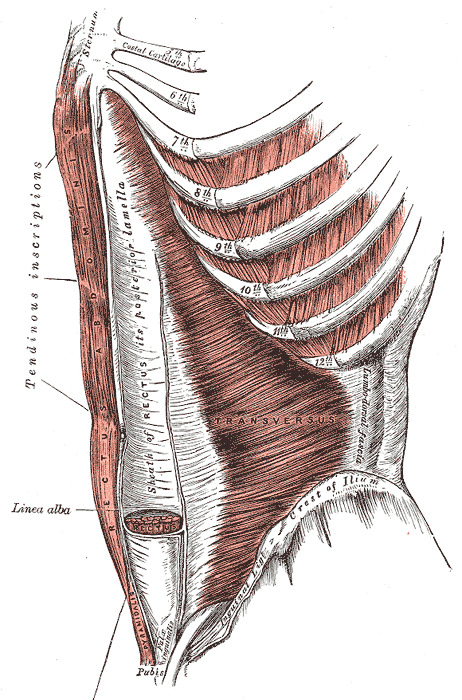
Not attaching directly to the lumbar spine, but playing a key role in truncal flexion are the abdominal muscles, the internal oblique, external oblique, and rectus abdominis. The external oblique muscle is most superficial, originating from the fifth to twelfth ribs and inserting at the linea alba, pubic tubercle, and anterior half of the iliac crest with its fibres running inferomedially. The internal oblique is deep to the external oblique. The internal oblique fibres run superomedially from the thoracolumbar fascia, anterior two-thirds of the iliac crest, and the lateral half of the inguinal ligament to the inferior borders of the tenth to twelfth ribs, linea alba, and pectin pubis via the conjoint tendon. The rectus abdominis originates from the pubic symphysis and crest and runs superiorly to the xiphoid process and the fifth to seventh costal cartilages. The rectus abdominis is interspersed by the intersectiones tendineae. These are tendinous bands that segment the muscle into smaller muscle bellies, giving the rectus abdominis its colloquial name of the “six-pack.” Less commonly noted, is that the tendons also provide structure against lateral forces and help the abdominal muscles resist the forces of motion on the lumbopelvic region. Another small muscle called the pyramidalis lies inferior to the rectus abdominis and is responsible for tensing the linea alba. The pyramidialis muscle is absent in 20% of the population. Deep to the internal oblique is the transversus abdominis muscle. The transversus abdominis originates on the internal surfaces of the seventh to twelfth costal cartilages, thoracolumbar fascia, iliac crest, and lateral third of the inguinal ligament with its fibres travelling horizontally to the linea alba.

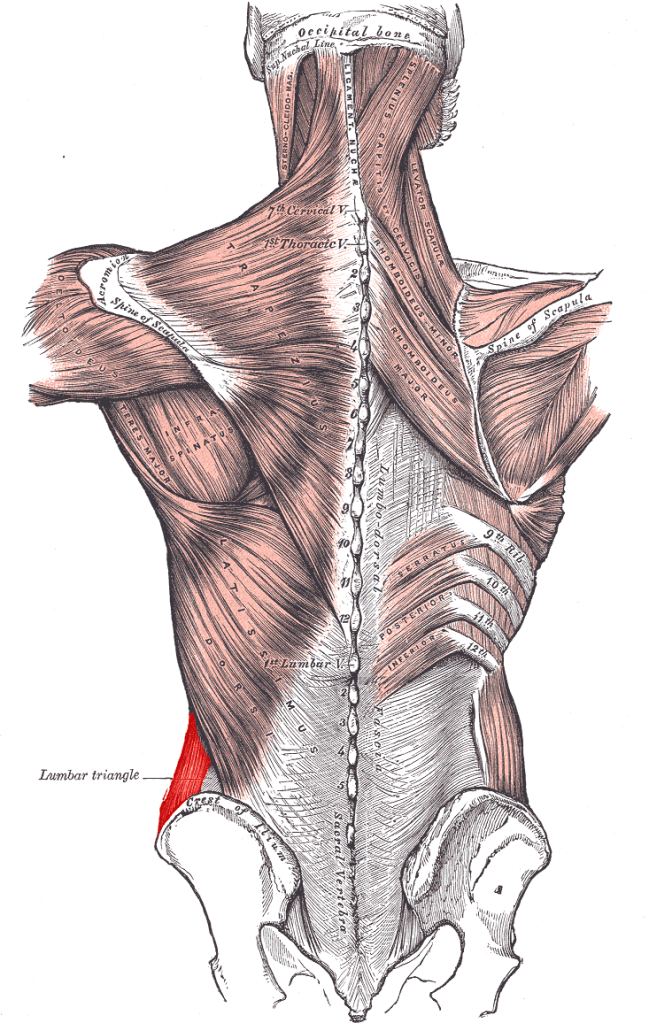
Laterally, the thoracolumbar fascia is a continuation of the longitudinal and transverse fibers of the aponeuroses of the internal oblique and transversus abdominis. It attaches to the lumbar vertebrae at the transverse and spinous processes (see the video below). The thoracolumbar fascia is a three-layer structure invaginating the erector spinae and transversospinales muscle groups between the posterior and middle layers, and the quadratus lumborum between the middle and anterior layers. The quadratus lumborum originates on the posterior border of the iliac crest and runs to the inferior border of the twelfth rib and transverse processes of the L1 to L5 vertebrae. In addition, the thoracolumbar fascia has attachments of the serratus posterior inferior, trapezius, latissimus dorsi, and gluteus maximus muscles. From the innovative perspective of the concept of the myofascial slings, visionaries like Dr. Andry Vleeming have seen the thoracolumbar fascia as an integral part of the human movement system connecting the upper appendages with the lower. Concerning SUP biomechanics, where the connection between hips and shoulders is necessary for efficient stroke mechanics, the thoracolumbar fascia, specifically, and myofascial slings and the core, generally, are key. I like the definition of the core given by Santana et al. (2015) as, “the torso between the ball and socket joints of the shoulders and hips.” As such, the thoracolumbar fascia is a key part of the core, but this is yet another case where the whole is greater than the sum of its parts.
Don’t Forget the Diaphragms
One last comment on the core regards the role of the horizontal diaphragms on spinal stability. Contrary to the complete torso definition of the core by Santana et al. (2015), another common conceptualization of the core is to conceive it as a cylinder. In this view, the thoracic and pelvic diaphragms are the respective top and bottom of the cylinder. The surrounding sides are made up of the lower back and anterior and lateral abdominal walls. Coordinated muscle contraction compresses the cylinder and increases intra-abdominal pressure, which is a contributory mechanism to overall spinal stability. The thoracic diaphragm has direct connections to the upper three lumbar vertebrae by way of the crus of the diaphragm. Whereas, the pelvic floor is attached to the base of the spine at the coccyx by way of the pubococcygeus. Both diaphragms have fascia connections to the lumbar spine structures.
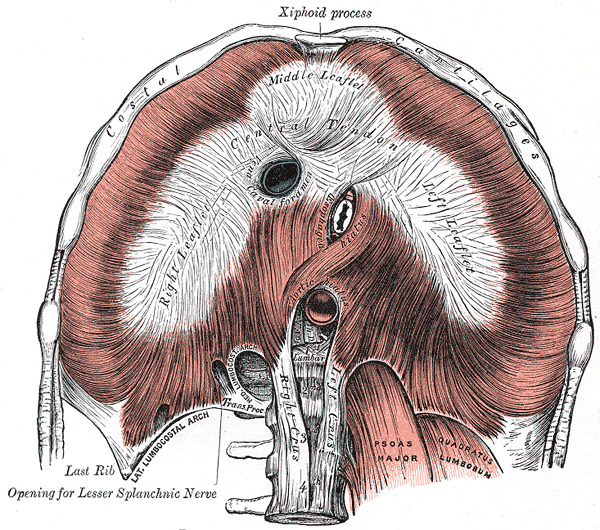
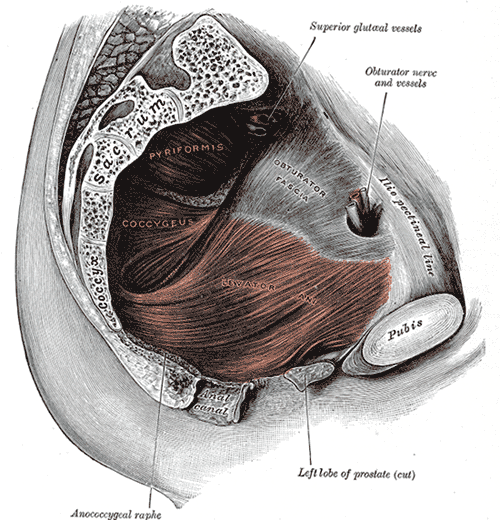
Source: https://commons.wikimedia.org/wiki/Gray%27s_Anatomy_plates
What About the Guts?
One other aspect of lower back health and function that is often neglected is the role of the viscera. Part of this is because it is a less studied and thus poorly understood aspect of anatomy. This stems from the complicated nature of both, neural and anatomical connections and relationships. Unfortunately, this creates an environment rife with pseudoscience at worst and unsubstantiated, but plausible claims at best. What we do know is that the viscera reside in the abdominal cavity and thus play a role in the intra-abdominal pressure/stability mechanism mentioned above. Anatomically, the viscera are lined by the peritoneum, which is a connective tissue cover anchoring the organs to the walls of the abdominal cavity. For example, the mesentery is an organ that attaches the intestines to the posterior abdominal wall in humans. The mesentery is formed by the double fold of the peritoneum and the root of the mesentery arises from structures in front of the vertebral column between the left side of the second lumbar vertebra and the right sacroiliac joint (see image below). While proof is lacking, there is some plausible conjecture that visceral function (e.g., digestion) may play a role in spinal biomechanics via these mechanical fascial links.
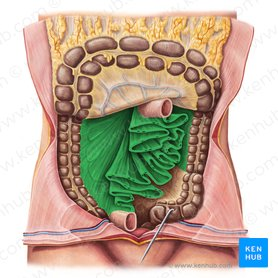
Source: https://www.kenhub.com/en/library/anatomy/mesentery
We also know that the viscera can refer pain to surrounding somatic structures through a process of somatovisceral convergence. Two examples of this that are popularly familiar are the low back pain associated with menstruation and arm pain associated with a heart attack. In both cases, the somatic pain experienced is not the consequence of somatic bodily harm or pathology. While general referral patterns for the various viscera have been reported, there is a lot of variation in the data sets. Look at the various schematics below from different sources to get an idea.
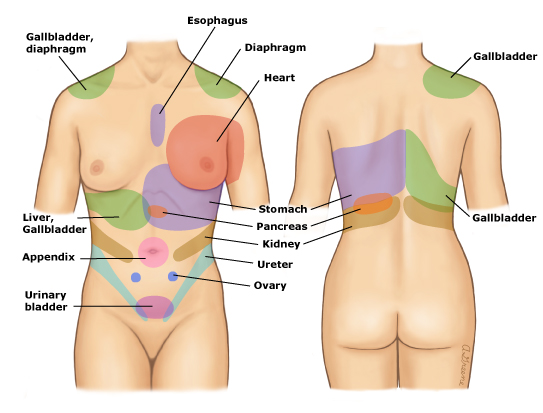


Sources: https://www.uptodate.com/contents/images/PC/61375/Referredpainpatterns.jpg
https://www.physio-pedia.com/File:Tumblr_lb03ir2vgL1qzr2i2o1_500.png
https://en.wikipedia.org/wiki/Referred_pain#/media/File:1506_Referred_Pain_Chart.jpg
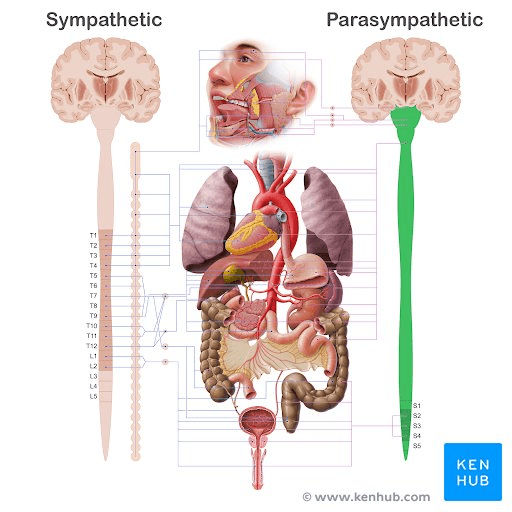
It is likely that the different patterns arise from individual differences in anatomy and sensory processing. A hypothesis is that referred pain results from neural convergence, where individual neurons receive input from many neurons within a network. While it is difficult to distinguish between viscerosomatic (i.e., referred pain) and somatic pain there are some general guidelines. True visceral pain tends to be a diffuse and poorly defined sensation and is often associated with marked autonomic phenomena (e.g., pallor, profuse sweating, nausea, gastrointestinal disturbances, changes in body temperature, blood pressure, and heart rate). The schematic below shows the two main divisions of the autonomic nervous system, the sympathetic and parasympathetic nervous systems (the third division is the enteric nervous system). The sympathetic nervous system is commonly referred to as the “fight or flight” system and the parasympathetic nervous system as the “rest and digest” or “feed and breed” system. The figure below highlights the autonomic innervation of the viscera. Noting the connections and general fight or flight and rest and digest roles of the respective systems helps to explain the associated autonomic phenomena of visceral pain listed above. A feature of visceral pain is that it can sensitize somatic tissues and thus alter their function, which is the implication for SUP biomechanics and the rationale for the inclusion in this discussion.
Movements
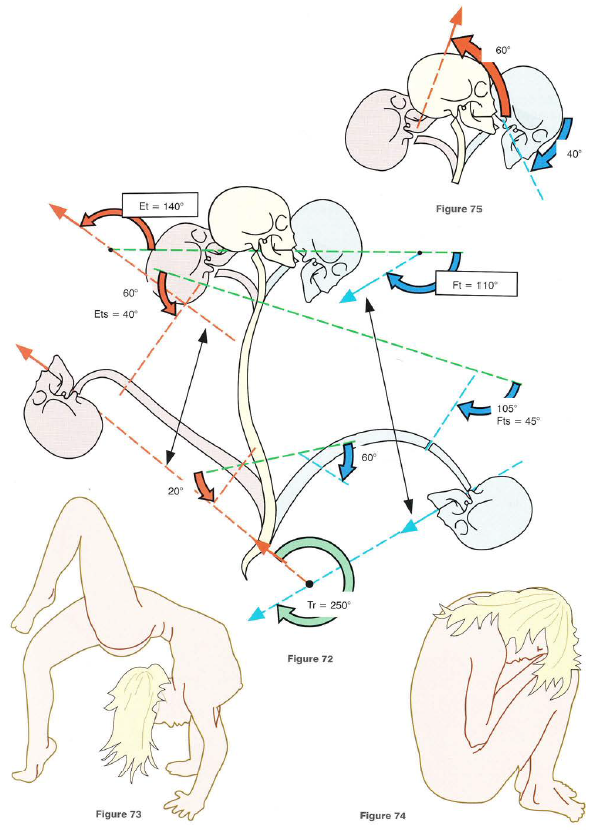
Source: Kapandji, I A. The Physiology of the Joints: Volume 3 The Spinal Column, Pelvic Girdle and Head, 2008.
The mobile spinal segments of the spine have six degrees of freedom. The lumbar vertebrae can undergo axial, lateral, and sagittal rotation in addition to axial, lateral, and anteroposterior translations. The ranges of motion are hard to quantify, both regionally and segmentally. Estimates are based on cadaveric and radiological studies.
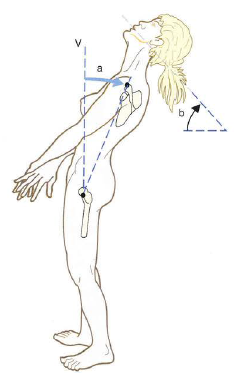
Flexion and extension take place in the sagittal plane. The lumbar spine collectively is reported to have approximately 60° of flexion and 20° of extension. Though, there is wide individual variation in their values. For comparison, the estimates for the thoracic spine are 45° of flexion and 40° of extension. Whereas the values for the cervical spine are 40° and 60° respectively. Collectively the entire spine has around 110° of flexion and 140° of extension.
Lateral flexion, or side bending of the spine, occurs in the coronal plane. For the lumbar spine, it is approximately 20°. The estimate for the thoracic spine is 20° and 35-45° for the cervical spine. Collectively the spine has approximately 75-85° of lateral flexion bilaterally.
Axial rotation of the spine occurs in the transverse plane. For the lumbar spine, it is estimated to be between 5-15°. The estimate for the thoracic spine is approximately 35° and ranges from 45-80° for the cervical spine. Collectively the spinal rotation exceeds 90° bilaterally.
The translational motions are even more difficult to quantify. Clinically, they are assessed by the quality of springiness in the vertebral structures and attempts to ascertain the accessory motions of spinal segments. These are the gliding motions of bones encompassed in arthrokinematics, that complement the osteokinematics. Suffice it to say that the vertebra should have some translational movement.
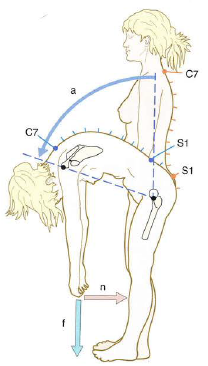
Often the movements of the spine do not occur in isolation. In fact, the spine is believed to undergo automatic rotation during lateral flexion, in a coupling movement, thought to result from the compression of the intervertebral discs and stretching of the ligaments (Kapandji, 2008). This phenomenon is seen clinically in scoliosis, where the spine has an abnormal curvature in the coronal plane accompanied by rotation. The rotation is most evident when the spine is flexed and is seen as an asymmetrical hump on one side. While my personal view is that we all have some degree of coronal curvature abnormality, true clinically relevant scoliosis is reserved for curvatures with a Cobb angle greater than ten degrees.

Both the mobility and stability of the lumbar spine are paramount to the function of the lumbopelvic-hip complex. Movement is necessary for proprioception, but that motion must be controllable for force production. It is the can’t fire a cannon out of a canoe analogy. The lumbopelvic-hip complex must efficiently transfer power from the lower to the upper extremities to harness the greater power production potential of the larger muscles of the lower body. In SUP, the transmission of force from the hips passes through the trunk (i.e., thorax and abdomen) to the shoulder girdle and ultimately water via the upper limbs and paddle. As such, the core needs to be mobile and stable to facilitate this power transfer.
A Recipe: Disc Herniation Anyone?
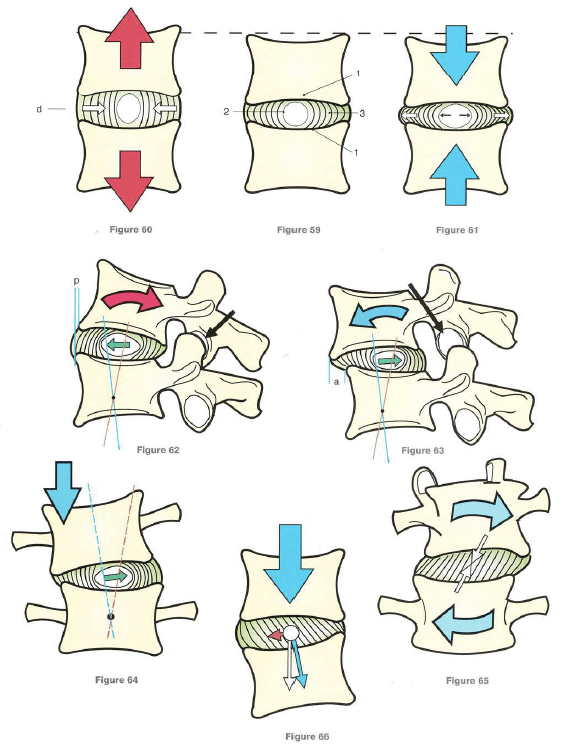
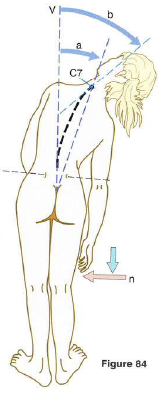
An extra note on lumbar axial rotation and lumbar disc pathology. As mentioned above, intervertebral disc herniation results when repetitive flexion under higher loads surpasses the stress tolerance of the annulus fibrosus’ laminal layers. As the collagen fibres delaminate the nucleus pulposus can migrate through to the outer layers of the lamina eventually creating a bulge. Generally, this is a gradual, repetitive strain process. There are several reasons why this occurs more commonly in the lumbar than the thoracic and cervical spine. One is that the lumbar intervertebral discs are larger with more substance to the nucleus pulposus. Because the lumbar spine supports more mass it must be larger and is subject to higher loads and forces. The greater vertebral size is hypothesized to be an adaptation to bipedalism. There is evidence to suggest that humans with lumbar spine anatomy more similar to our evolutionary ancestors are more susceptible to an intervertebral disc injury, the “ancestral shape hypothesis.” Another reason is that second to the cervical spine region, the lumbar spine segments are the next most mobile. Again, this motion translates to more stress on the intervertebral discs. The cervical and thoracic spine have the added protection of the uncinate processes and rib cage, respectively to limited motion and disc herniation. Lastly, the position of the axis of rotation of the lumbar spine does not coincide with the centre of the disc. Due to the orientation of the zygapophyseal joints the axis of rotation is posterior to the disc (see image below). This results in more lateral glide of the vertebra during rotation and greater shearing force. The combination of these intrinsic factors results in greater susceptibility to a disc injury in the lumbar spine. These non-modifiable factors highlight the importance of optimum biomechanics for injury risk reduction by taking control of modifiable factors.
Lumbar Plumbing: Vasculature and Lymphatics


Sources: https://en.wikipedia.org/wiki/Lumbar_arteries#/media/File:Gray1120.png
https://pressbooks.bccampus.ca/advancedanatomy1sted/chapter/nerves-blood-vessels-and-lymph-3/
https://www.uptodate.com/contents/image?imageKey=SURG%2F51087
https://www.researchgate.net/figure/Tributaries-of-the-inferior-vena-cava-and-lumbar-veins-4_fig1_283441416
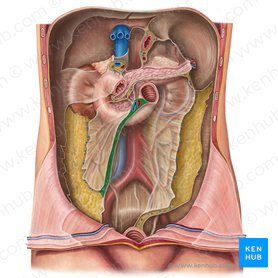
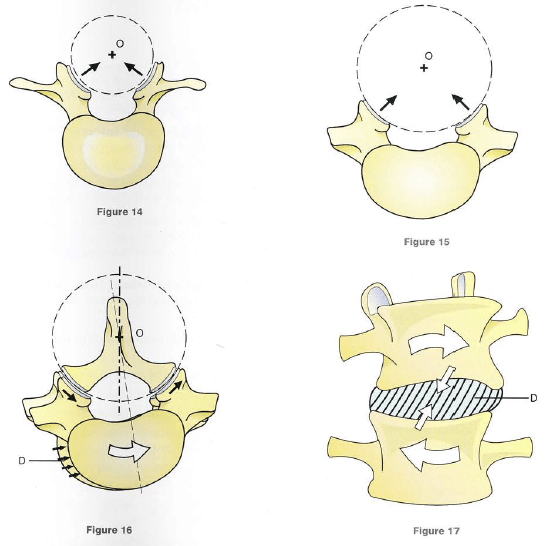
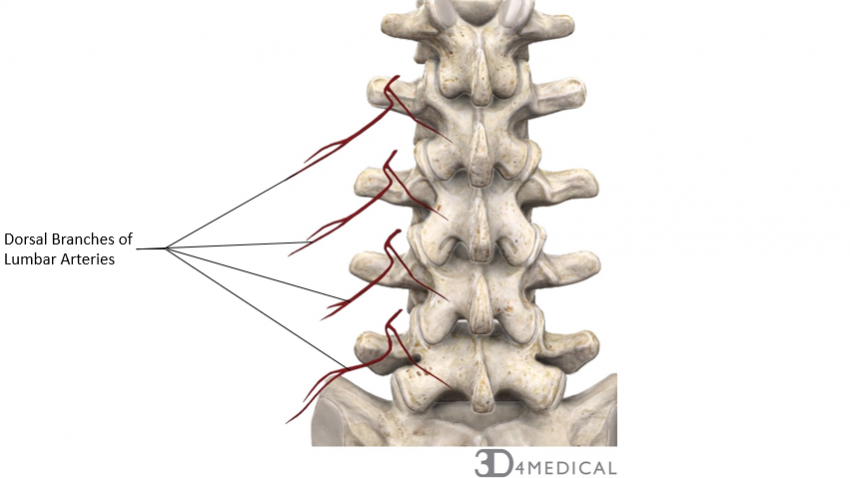
Specific to the lumbar spine, four pairs of lumbar arteries originate from the abdominal aorta. These paired arteries travel posteriorly along the vertebral bodies to supply each vertebra. The arteries also supply blood to the adjacent musculature (e.g., transversus abdominis and internal oblique). Blood flow to the spinal cord is rich, stemming from three main longitudinal arteries. A single anterior spinal artery supplies the anterior two-thirds of the cord. Two posterior spinal arteries supply the posterior one-third of the cord. Several anterior and posterior radicular arteries provide collateral blood supply to the vertebral column. The radicular arteries run along with the ventral and dorsal nerve roots and supply them with blood. The artery of Adamkiewicz is the largest radiculomedullary artery and provides vascular supply to the lumbar spinal cord.
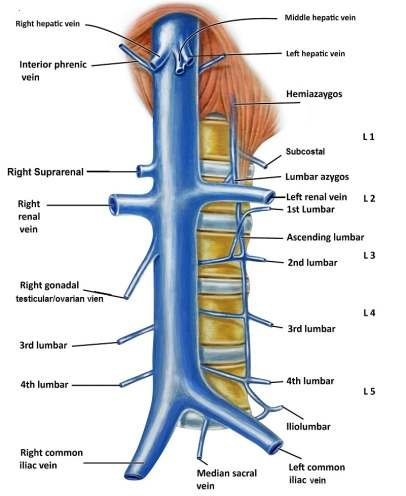
The venous drainage of the spinal cord is accomplished by one to three anterior and posterior spinal veins, respectively. These veins drain into the internal and external vertebral venous plexuses, which empty into the systemic segmental veins, that is, the posterior intercostal, subcostal, and lumbar veins.
An extensive system of lymphatics in the lumbar region is responsible for draining lymph from the lower limb and pelvis. These lymph nodes are present along the inferior vena cava and aorta. The lumbar lymph nodes receive drainage from the common iliac nodes and deliver this lymph to the thoracic trunk.
The lymphatics of the spinal cord are indirectly connected to the general lymphatic and venous systems. They open into the subarachnoid space.

The vascular and lymphatic systems of the body are important for both performance and recovery. Together they help to regulate nutrient supply, waste removal, metabolism, immunity, and inflammation. However, generally, they are viewed from a medical/pathoanatomical perspective.
Wow, that was a lot! And it got into the weeds a little bit(😬). Stay tuned for Lower Back Volume 2, where I will cover more SUP-specific lumbar spine mechanics…

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
2 thoughts on “SUP Biomechanics: Lower Back Volume 1”