
Anatomy 102
Saturday, January 22, 12022 HE
A word of warning. My interest in anatomy started in high school when I got into strength training. Anatomy was then my favourite subject during my undergraduate degree in Human Kinetics. It remained my favourite subject during my Physical Therapy studies. It was still my favourite area of study when I completed a Diploma in Manual Osteopathy. All this is to say that this may go into too much detail for the less anatomically enthused.
Full disclosure, I am a licensed physical therapist and manual osteopathic practitioner, but the following is purely for informational purposes. For formal guidance concerning your stand up paddleboard (SUP) biomechanics, it may be in your interests to seek out the aid of a licensed/qualified professional. If you are experiencing pain with physical activity, exercise a degree of caution when evaluating the nature of your symptoms. Pain with movement or exertion can be a normal symptom, but it may also signal something more nefarious. Use your own personal judgement, but if in doubt, err on the side of caution for a proper evaluation licensed/qualified medical professional.
- Anatomy 102
- SUP Biomechanics Overview
- Mobility and Stability Subsystems
- What’s in a Hip? Bones and Joints.
- More of the Passive Stuff: Inert Tissues
- The More Active Stuff: Nerves and Muscles of the Hip Complex
- What Does it All Do? Motions of the Hip.
- Blood Flow and Drainage
This post is my fourth on SUP biomechanics. The first post was a general overview of SUP biomechanics, which you can see here. For the second one, on shoulder anatomy, click here. And for the third, on SUP shoulder biomechanics, click here.
SUP Biomechanics Overview
Stand up paddleboarding is a quickly growing aquatic recreational and sporting activity. It is easily accessible to most people since it requires minimal equipment and is easy to learn. It can be practiced on almost any body of water and provides a low impact, full-body physical challenge, suitable for all ages and skill levels. As with any activity, SUP has risks (see this post for general SUP safety guidelines). Concerning musculoskeletal injuries specifically, a 2017 study by Furness and colleagues revealed that the shoulder/upper arm was the most frequently injured body location (32.9% of all injuries). Hence why my first posts on SUP biomechanics focused on the upper extremity. In the study by Furness and colleagues, the lower back was the next, most commonly reported injury site, at 14.3% of all injuries. The hip/buttock only accounted for 3.7% of all the injuries reported, but as we will see, its relation to the back is significant.
Schram and colleagues’ 2019 paper compared the stroke biomechanics of experienced and inexperienced paddlers. The study’s main finding was that experienced paddlers used less shoulder movement and more hip movement. The data was collected on a KayakPro SUP ergometer, and it did not look at injuries specifically. It only compared the biomechanics between the two groups. You can see animations of two representative paddlers (one experienced, one inexperienced) created from their data in the video clip below. The experienced paddler on the left demonstrates much more full-body movement than the inexperienced paddler on the right. Notice how much more the experienced paddler’s pelvis, and therefore hips move.
As I did for the shoulder, I would like to cover some hip anatomy before delving into the biomechanics (for more details, see Byrne et al., 2010 and Bowman et al., 2010).
Mobility and Stability Subsystems
Again, Panjabi’s (1992) landmark theoretical model for spinal stability is a great framework to conceptualize the stability of the joint structure. Simply, he proposes that three subsystems (neural, passive, and active) govern the overall biomechanical control of a joint. Below is a schematic of Panjabi’s model and an expanded version by Hoffman and Gabel (2013) highlighting the expression of movement (i.e., mobility and stability). This model applies to all the articulations in the body. As was the case for the shoulder, for the hip to be stable and function, there must be cooperation between the various subsystems contributing to mobility and stability.

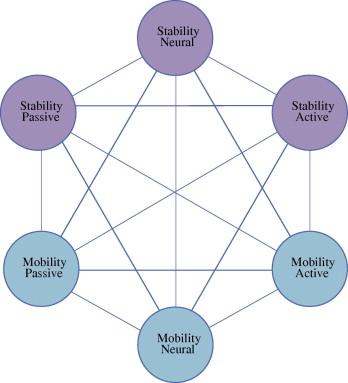
Source: Hoffman, J., and P. Gabel. “Expanding Panjabi’s Stability Model to Express Movement: A Theoretical Model.” Medical Hypotheses, vol. 80, no. 6, 2013, pp. 692–697., https://doi.org/10.1016/j.mehy.2013.02.006.
What’s in a Hip? Bones and Joints.
The hip proper is a true ball-and-socket joint capable of a large range of motion. It is the second-most mobile joint in the body, next to the shoulder. However, unlike the shoulder, the hip is inherently more stable due to its osseous structure. The acetabulum of the coxofemoral joint is a much deeper fossa than the glenoid of the glenohumeral joint. In a broader context, like the shoulder complex or girdle, the hip can be looked at as a complex, or girdle, including both innominate bones and the sacrum attached via the sacroiliac joints. The innominate or hip bone develops from eight ossification centres, the three primary ones being the ilium, ischium, and pubis. The hip is part of the appendicular skeleton but is directly connected to the axial skeleton. Complicating this complexity further would be extending the complex to include the adjacent spinal structures, the so-called lumbopelvic-hip complex. In the same way that the shoulder is intimately interconnected with the cervical and thoracic spine, the same holds true for the hip and the lumbar spine.
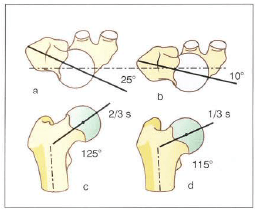

Source: Kapandji, I A. The Physiology of the Joints: Volume 2 The Lower Limb, 2011.
Another aspect of the osseous anatomy of the hip is its angles. Two that I will briefly cover are the version of the femoral neck (anteversion or retroversion) and the femoral neck angle (or angle of inclination). Femoral version is generally used in medicine as a pathological term. It is the degree to which the neck of the femur is rotated forward in the transverse plane to a line through the femoral condyles. However, a diagnosis is generally made from a clinical assessment of gait and osteokinematics. We all have some degree of version with the estimated physiological average being 8 degrees (Litrenta and Domb, 2018). However, the reported range was -23 to 63 degrees. Version is on a spectrum, where at the extremes it can be a problem.
The femoral neck angle is in the coronal plane and is the angle of the neck of the femur to the long axis of the femoral shaft. The angle is generally between 120 and 135 degrees. When the angle is less than 120 degrees it is referred to as coxa vara. This is often associated with genu valgum (or knock-knees). When the angle is 140 degrees or greater it is termed coxa valga and is often associated with genu varum (or bow legs).
At the same time, a similar morphotypic presentation as above can be seen with changes in the orientation of the acetabulum. The functional implication is that if someone’s hip(s) is at the extreme of the spectrum osteologically, it is not likely to change shape or function.
The coxofemoral joint has six degrees of freedom, but most of its motion is rotational and not translational. The hip can be subject to instability which can ultimately lead to injury. For a great description of how instability can lead to excessive shear or frictional forces at the joint surface and the development of osteoarthritis see here in Fetto (2019). The hip can also be subject to impingement, labral injury, as well as various muscle strains and ligamentous sprains.
More of the Passive Stuff: Inert Tissues

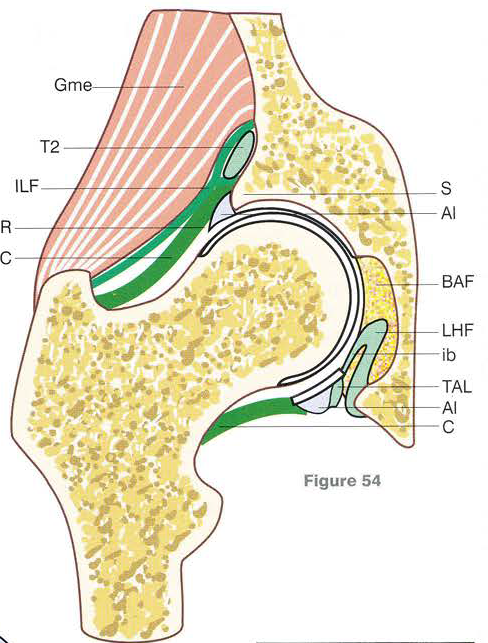

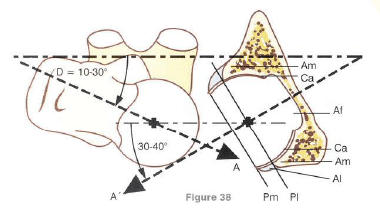
Source: Kapandji, I A. The Physiology of the Joints: Volume 2 The Lower Limb, 2011.
Image 1: (AL) acetabular labrum, (IPN) iliopubic notch, (AN) acetabular notch, (TAL) transverse acetabular ligament, (T1) straight head of rectus femoris tendon, (T2) reflected head of rectus femoris tendon, (T3) recurrent head of rectus femoris tendon, (RF) rectus femoris tendon, (LHF) ligament of head of femur (aka. ligamentum teres), (pi) posterior ischial bundle, (ap) anterior pubic bundle, (ib) intermediate bundle
Image 2: (Gme) gluteus medius, (C) capsule, (ILF) iliofemoral ligament, (T2) reflected tendon of rectus femoris, (BAF) back of the acetabular fossa, (AL) anterior labrum, (TAL) transverse acetabular ligament, (LHF) ligament of head of femur, (ib) intermediate bundle, (S) supra-acetabular ridge
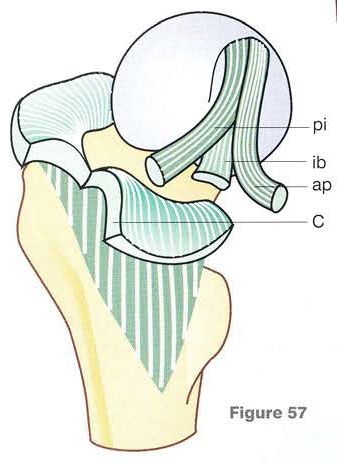
Image 3: (C) capsule, pi) posterior ischial bundle, (ap) anterior pubic bundle, (ib) intermediate bundle
Image 4: (RF) rectus femoris tendon, (R) perimarginal circular recess (aka. Rouviere recess), (AL) anterior labrum, (T) tent of the ligament of head of femur, (LHF) ligament of head of femur, (C) capsule, (TAL) transverse acetabular ligament
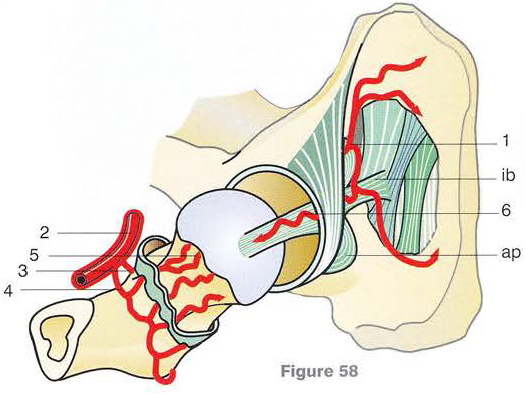
Image 5: (ap) anterior pubic bundle, (ib) intermediate bundle, (1) posterior branch of the obturator artery, (2) deep femoral artery, (3) anterior and (4) posterior circumflex arteries, (5) capsular branches of circumflex arteries, (6) artery of the ligament of head of femur
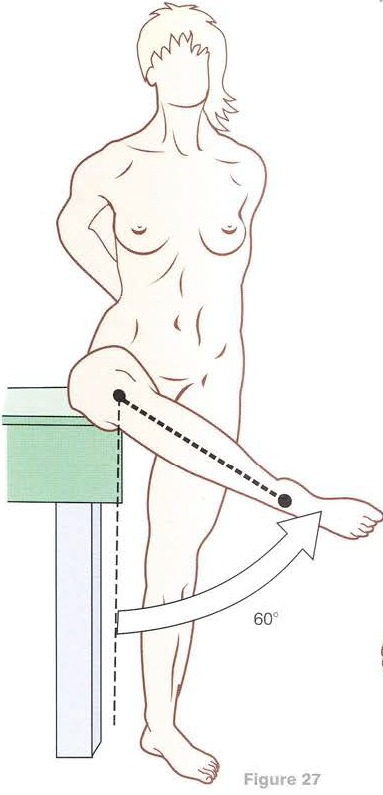
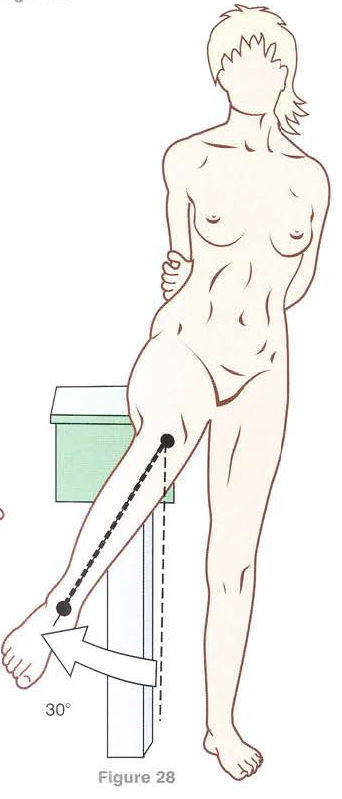
The innate stability of the coxofemoral joint arises from its deep acetabular fossa. The depth of the acetabulum also controls the absolute limits of the joint’s range of motion. Generally, normal hip ranges of motion are as follows: flexion (120-150°), extension (10-20°), abduction (45-80°), adduction (25-30°), medial rotation (15-40°), and lateral rotation (35-50°). These values are general guidelines, but variations between individuals outside of these values occur. The hip is also capable of circumduction, a combination of these movements.
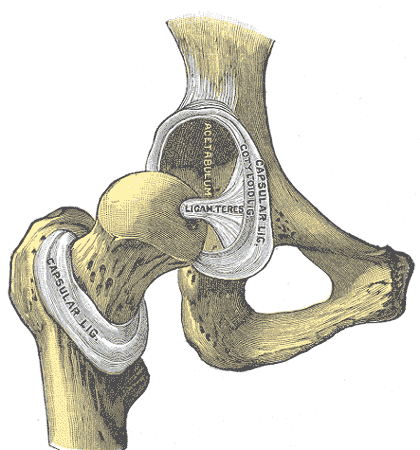
The hip joint has a labrum. The labrum increases the articular surface area by approximately 22% and the volume of the acetabulum by 33%. The labrum may also help to limit extreme ranges of motion, acting as a bumper. Like in the shoulder, it is hypothesized that the labrum seals the joint, enabling increased hydrostatic fluid pressure, aiding with synovial lubrication and resistance to joint distraction. The acetabular labrum is continuous with the transverse acetabular ligament which, crosses the acetabular notch.

Sources: https://en.wikipedia.org/wiki/Hip#/media/File:Gray341.png
https://en.wikipedia.org/wiki/Hip#/media/File:Gray342.png
The acetabulum is lined with articular cartilage (hyaline cartilage) formed by chondrocytes. The chondrocytes produce the two critical components of the cartilage, collagen and proteoglycan. The femoral head is also covered in hyaline cartilage. Thus, both surfaces are lined by multiple highly organized layers of hyaline cartilage, the properties of which provide stress-shielding protection to the hip joint (Bowman et al. 2010; Fetto, 2019)*. The geometric orientation of the articular cartilage is also optimized for load transfer, with the thickest portions aligned with the areas loaded during upright stance and gait. The cartilage is thickest at the ventral-cranial surface of the acetabulum and the ventrolateral surface of the femoral head. The cartilage density decreases concentrically from these points. Along with the subchrondral bone, the cartilage works synergistically to manage load transmission through the hip. The fovea capitis is a small depression in the head of the femur that remains unloaded and is the attachment site for the ligamentum teres femoris. Generally, the ligamentum teres is not believed to contribute significantly to the stability of the joint. Rather, it may aid with blood supply to the femoral head as it carries the acetabular branch of the obturator artery within it. The ligament is intracapsular and covered with the synovium, so it is intra-articular yet extra-synovial.
*As a sidenote tangent on joint surfaces, I recently listened to this episode of the BBC’s The Curious Cases of Rutherford and Fry: The Slippery Situation. It is all about the science of Tribology, which is the study of friction and lubrication between surfaces. Worth a listen to learn how much friction costs the economy, what is the most dangerous food item to slip on at the supermarket, and why you should never spray a car crash involving a truck carrying hagfish with water, among other curiosities.

Source: https://www.theatlantic.com/science/archive/2019/01/hagfish-slime/581002/

Sources: https://en.wikipedia.org/wiki/Hip#/media/File:Gray339.png
https://en.wikipedia.org/wiki/Hip#/media/File:Gray340.png
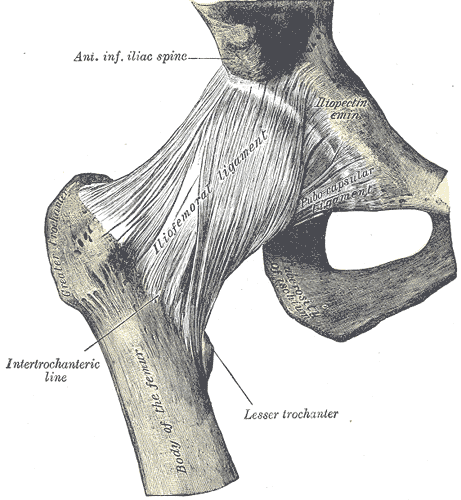
There are three extracapsular ligaments for the hip that are thickenings of the joint capsule. These ligaments act as primary static stabilizers. The strongest ligament is the iliofemoral ligament. It spirals from its proximal attachment to the area between the anterior inferior iliac spine and acetabular rim to the intertrochanteric line of the femur. Its main role is to limit extension and lateral rotation of the hip. It also prevents posterior pelvic tilt in an upright stance conserving muscle activation.
The ischiofemoral ligament reinforces the posterior aspect of the joint capsule. It originates from the ischial rim of the acetabulum and follows the iliofemoral ligament as it twists around the femoral head to insert onto the superolateral aspect of the femoral neck, medial to the base of the greater trochanter. The ischiofemoral ligament limits medial rotation and adduction with the hip in flexion.
The pubofemoral ligament is inferior and posterior to the iliofemoral ligament and blends with its medial edge. The pubofemoral ligament contributes to the strength of the anteroinferior portion of the capsule.
The inner lining of the articular capsule is a synovial membrane. This membrane produces synovial fluid to lubricate the articular surfaces. There are also bursae within the capsular complex.
Centration of the coxofemoral joint is necessary for optimal function. As a true ball-and-socket joint, the hip is inherently more stable and thus centrated. However, muscular activity is still needed for proper joint centration.
The More Active Stuff: Nerves and Muscles of the Hip Complex
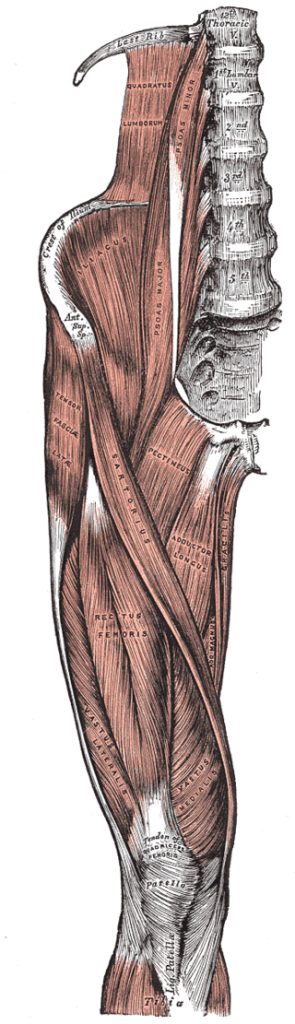


Sources: https://commons.wikimedia.org/wiki/Gray%27s_Anatomy_plates
https://www.statpearls.com/ArticleLibrary/viewarticle/32250
The mobility of the hip complex is ultimately controlled by the nervous system, regulating 22 muscles that directly act on the joint. Control is governed voluntarily (somatic nervous system) and involuntarily (autonomic nervous system). The nervous system requires a robust amount of proprioceptive information. Proprioceptive information transmits to the nervous system from mechanoreceptors located in the tissue. The mechanoreceptors are specialized sensors in tissues that respond to compression or distraction.
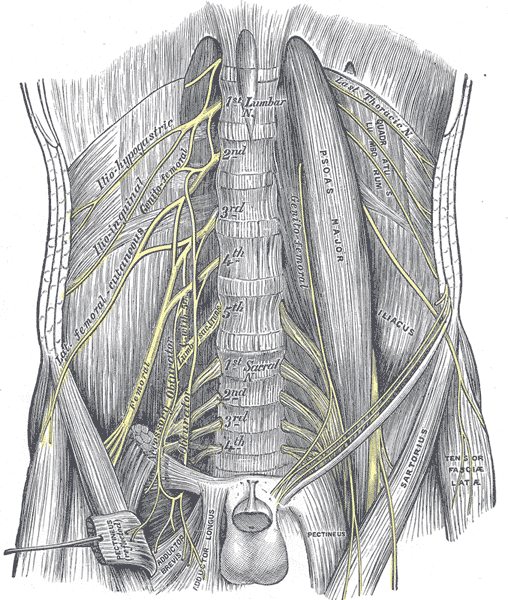

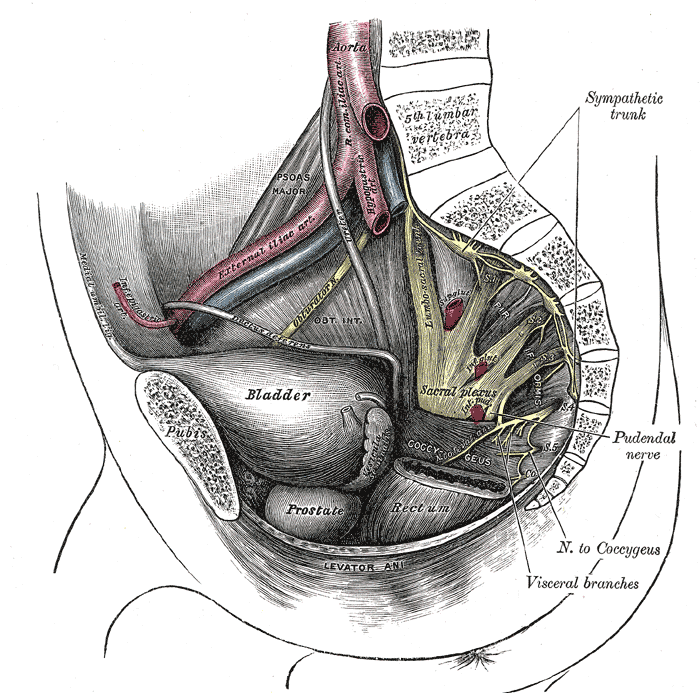
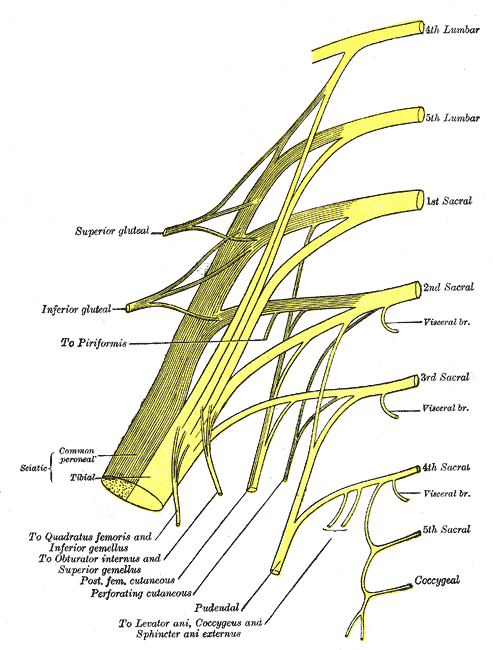
Source: https://commons.wikimedia.org/wiki/Gray%27s_Anatomy_plates
The innervation of the coxofemoral joint has separate sources for the anterior and posterior portions. Ultimately the innervation arises from the lumbosacral plexus. The anteromedial portion of the joint is innervated by articular branches of the obturator nerve. While the anterior aspect is supplied by branches of the femoral nerve. The posterior aspect of the joint is innervated laterally by branches of the superior gluteal nerve. The medial contributions are from articular branches of nerves to quadratus femoris and articular branches from the sciatic nerve. It is this complex, shared innervation that makes the diagnosis of hip pathology complicated. Because of the mixed circuitry of the hip, referred pain/symptoms or radicular pain/symptoms can originate from the back or manifest in the hip, back, thigh, or knee.
To wrap your head around referred pain, consider what I think is the most commonly known source that almost everyone has experienced, brain freeze. When eating something very cold, the blood vessels surrounding the soft palate of the mouth undergo rapid vasoconstriction and vasodilation. This stimulates nerves supplying the area. Rapid vasodilation causes the tissue to stretch and can be interpreted as pain by the nervous system. The nerves innervating the soft palate are branches of the trigeminal nerve, which also has branches to the face and meninges (the connective tissue to the inside of your head). It is this shared innervation and the body confusing the incoming signals that are the explanation for brain freeze.
The same mixing of signals can happen elsewhere in your body. For the hip, sensations between the back, thigh, and knee can be confused with the hip since the neurological pathways overlap. For example, the obturator and femoral nerves both arise from branches of the lumbar plexus. The femoral nerve arises from the dorsal divisions of the ventral rami of the second, third, and fourth lumbar nerves (L2, L3, and L4). Whereas, the obturator nerve arises from the ventral divisions of the L2, L3, and L4. The sclerotome of the thigh is often attributed to L3, the knee is innervated by the femoral nerve, and spinal segments have shared innervation from the ventral rami for the intervertebral discs and ligaments and dorsal rami for the posterior elements (Bogduk, 1985). All this is to say that symptoms/sensations arising in the back or legs can be challenging to determine without a good understanding of the interconnected neurological relationships. This is without even considering the innervation of the hip that arises from the sacral plexus.


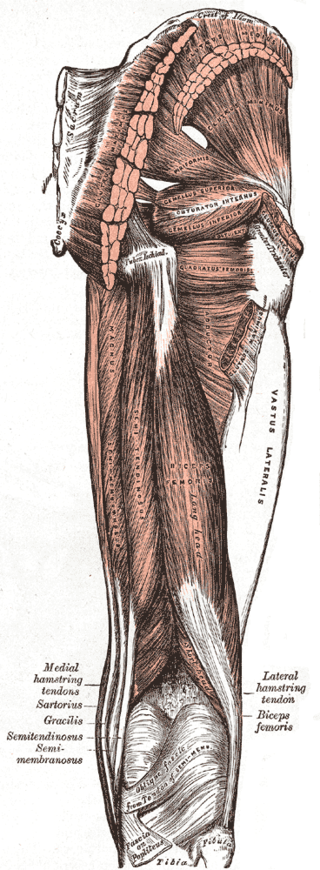
Sources: https://en.wikipedia.org/wiki/Lateral_rotator_group#/media/File:Posterior_Hip_Muscles_1.PNG
https://www.visiblebody.com/blog/learn-muscle-anatomy-lateral-rotators
The lateral rotators of the hip function similar to the rotator cuff of the shoulder. The concavity compression mechanism we discussed for the shoulder is also at play for the hip. Due to the greater stability afforded the hip from its osseous structure the concavity compression mechanism plays a lesser role in maintaining joint centration. When the larger multiarticular muscles of the hip contract, they are less likely to move the femur out of alignment within the acetabulum. Particularly, in a normal hip where there is a deep hip socket. However, in a condition like hip dysplasia, where the hip socket does not form completely or is misaligned, the role of the lateral rotator group becomes much more important to the stability of the joint.
What Does it All Do? Motions of the Hip.


Source: Kapandji, I A. The Physiology of the Joints: Volume 2 The Lower Limb, 2011.
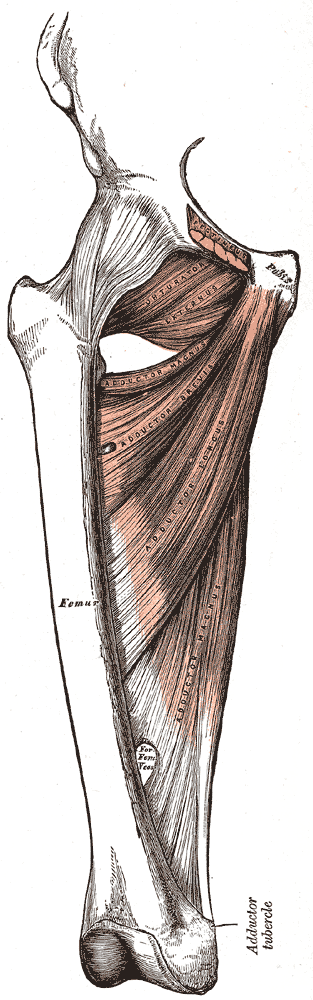
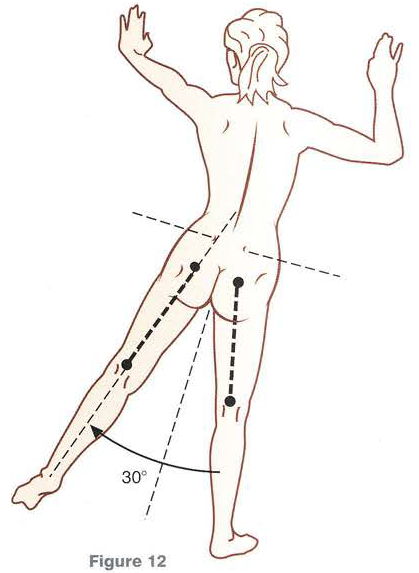
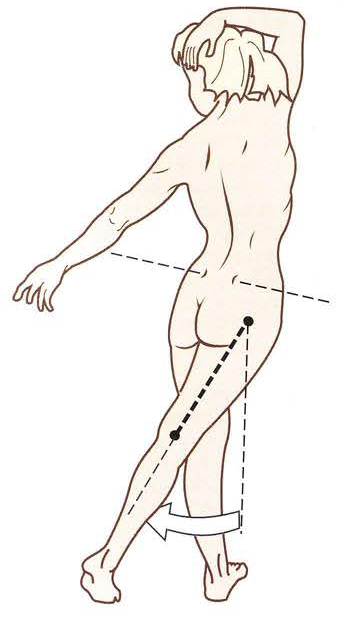
As mentioned, the hip is the second most mobile joint of the body. The hip is capable of flexion, defined as bringing the lower limb anteriorly in the sagittal plane. The normal range of hip flexion is between 120 to 150 degrees. The main flexor of the hip, the iliopsoas muscle, is comprised of the psoas major and minor, and the iliacus. Hip flexion is also aided by the sartorius, rectus femoris, and tensor fasciae latae (aka. TFL). Extension, defined as bringing the lower limb posterior in a sagittal plane, has a normal range of motion of 10 to 20 degrees. The gluteus maximus is the largest and most powerful extensor of the hip. Hip extension is also assisted by the gluteus medius (middle and posterior fibers), adductor magnus (anterior and posterior heads), and hamstring (semimembranosus, semitendinosus, and biceps femoris (long head)). Medial rotation (aka. internal rotation) is defined as rotation toward the midline along a vertical axis. The normal medial rotation range of motion is 15 to 40 degrees, but it is dependent on the degree of hip flexion. The amount of flexion (or extension) at the hip alters the ligamentous and muscle fibre orientation of the hip tissues and their respective tensions and actions. The muscles responsible for medial rotation include gluteus minimus (anterior fibers), gluteus medius (anterior fibers), tensor fasciae latae, adductor longus, adductor brevis, pectineus, and adductor magnus (posterior head). Lateral rotation (aka. external rotation) is defined as rotation away from the midline along a vertical axis. The normal range of lateral rotation is 35 to 50 degrees. Lateral rotation is achieved primarily by the gluteus maximus. But it is also assisted by the obturator internus, gemellus superior and inferior, and quadratus femoris, as well as secondarily by the gluteus minimus (posterior fibres), obturator externus, piriformis, and biceps femoris (long head). Abduction of the hip is defined as bringing the lower limb away from the midline in the coronal plane. The normal range of motion is 45 to 80 degrees. Abduction is performed primarily by the gluteus medius (all fibres), gluteus minimus (all fibres), and tensor fasciae latae. Abduction is assisted by the gluteus maxiumus (upper fibres), piriformis, and sartorius. Adduction is defined as bringing the lower limb toward the midline in the coronal plane. The normal range of motion is to zero degrees in anatomical position. Adduction of 25 to 30 degrees can be achieved when coupled with some flexion or extension to cross the midline. The primary adductors of the hip are the adductor group (pectineus, gracilis, adductor brevis, adductor longus, and adductor magnus (anterior and posterior heads)). Hip adduction is assisted by the biceps femoris (long head), gluteus maximus (posterior fibres) quadratus femoris, and obturator externus.
For a list of the primary and secondary hip muscles for each action see this table. One thing to keep in mind is that the actions of a muscle are generally reported for open kinetic chain movements and with the start or reference point of anatomical position. In open kinetic chain movements, the distal aspect of the limb segment is free to move. However, if the motion is a closed kinetic chain or the actions start outside of anatomical position then the action of a muscle can be reversed. For example, the gastrocnemius muscle is generally considered to flex the knee and plantarflex the ankle. However, if the foot is planted on the ground and the knee is flexed, then the action at the knee can be reversed and a shortening of the gastrocnemius will extend the knee joint. A similar phenomenon can take place for the hip, where the hip flexors can pull the hip into extension.
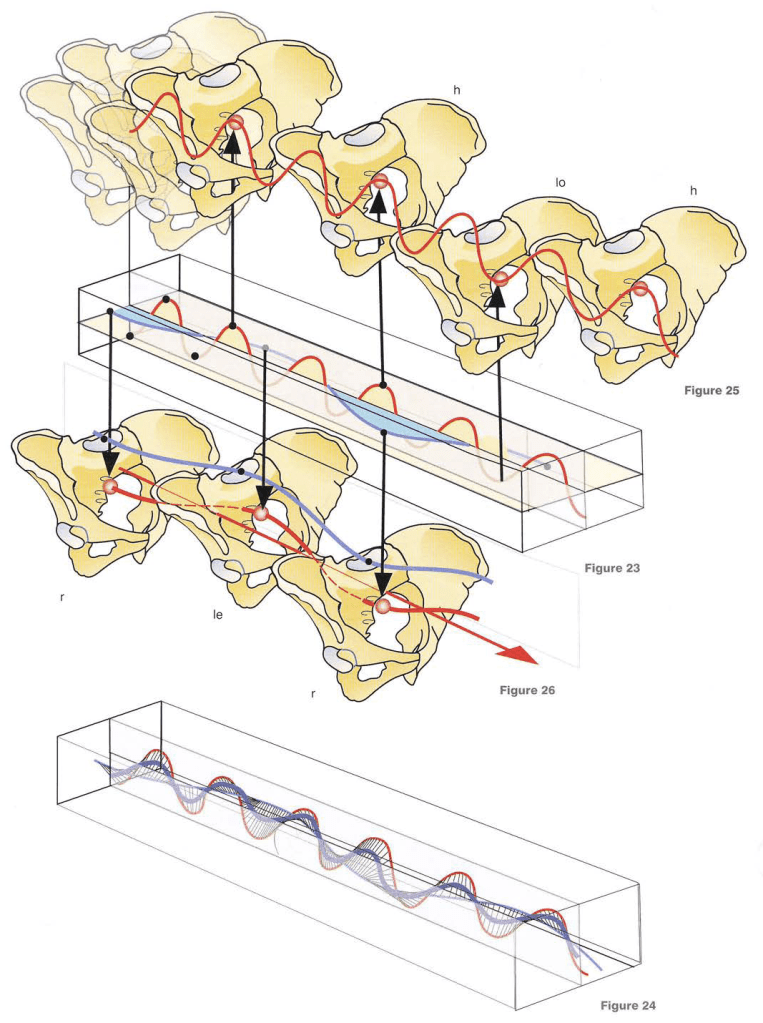
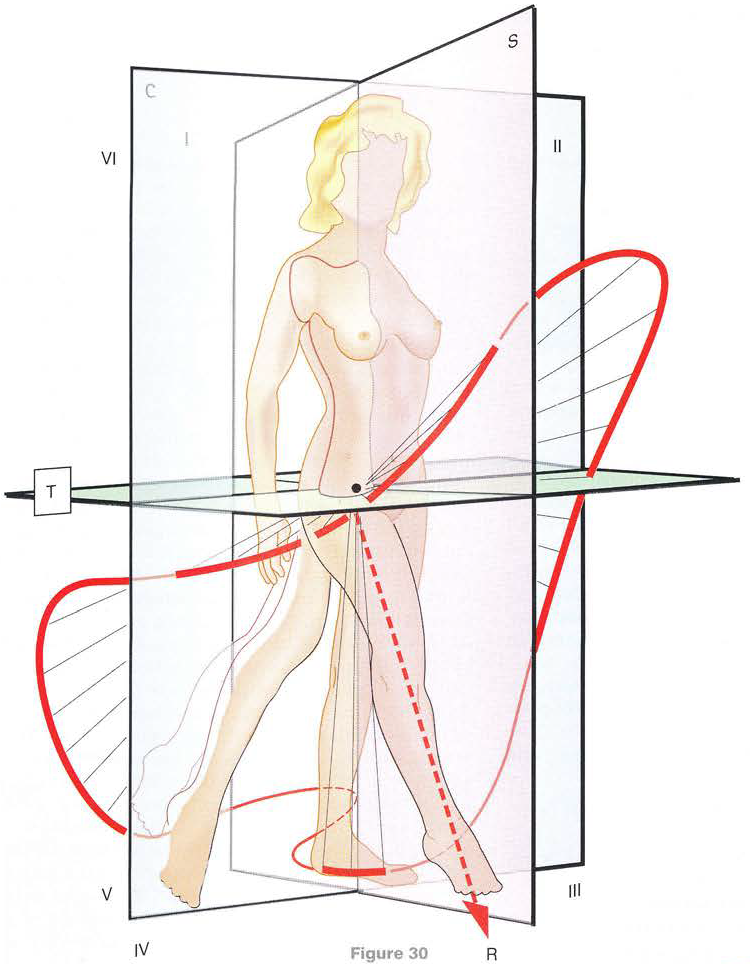
As in the shoulder where the scapula and shoulder girdle played a role in motion and stability, so too is the case for the hip and pelvic girdle. While the sacroiliac and pubic symphysis joints of the pelvis are much more stable than their anatomical correlates of the scapulothoracic junction, acromioclavicular, and sternoclavicular joints, they do still have motion. The innominate of the pelvis is capable of anterior and posterior rotation via the sacroiliac joint. In addition, the sacrum can move relative to the innominate bones into nutation or counternutation. The motions are coupled with inflare and outflare of the innominates due to the plane of the sacroiliac joint. Globally, the pelvis as a unit is capable of anterior and posterior pelvic tilt, lateral tilting in the coronal plane, and rotation in the transverse plane. Global motion of the pelvis often couples with countermovements in the lumbosacral and coxofemoral joint, thus involving the entire lumbopelvic-hip complex. The degree of global movement of the pelvis and the difference between experienced and inexperienced paddlers is very evident in the SUP biomechanics video above.
Both the mobility and stability of the lumbopelvic-hip complex are paramount to the direct function of the hip. It is the can’t fire a cannon out of a canoe analogy. The hips are the major power generators of the body. The largest muscle in the body, the gluteus maximus, crosses the joint. In SUP, the transmission of this force from the hips passes through the trunk (i.e. thorax and abdomen) to the shoulder girdle and ultimately water via the upper limbs and paddle. As such, the core or trunk needs to be mobile and stable to facilitate this transfer of power. Perhaps this will be another post as it is a topic unto itself…
Blood Flow and Drainage
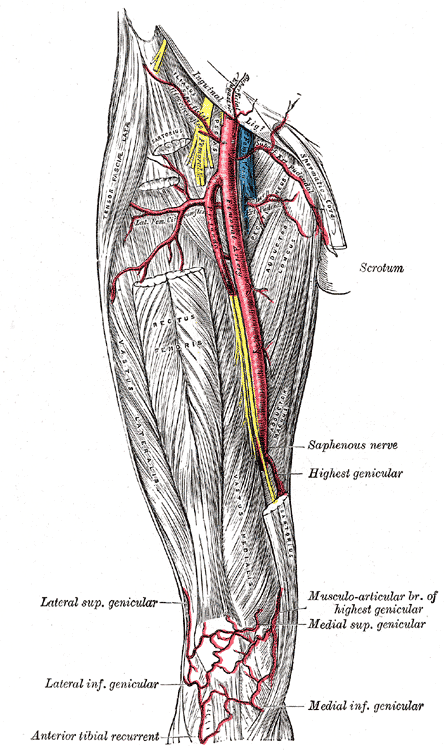
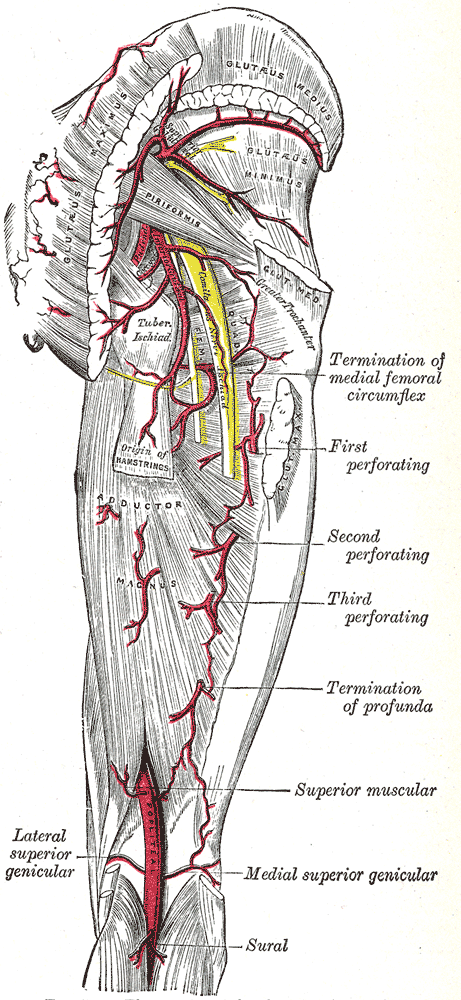
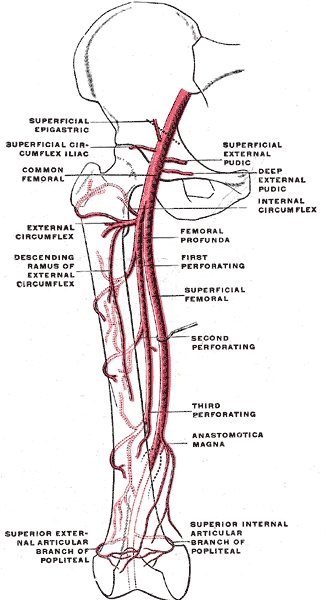

Sources: https://commons.wikimedia.org/wiki/Gray%27s_Anatomy_plates
https://en.wikipedia.org/wiki/Obturator_artery#/media/File:Internal_iliac_branches.PNG
There are numerous variations in the blood supply to the coxofemoral joint. The most common variant results in blood supply coming from the medial circumflex femoral artery with the lateral circumflex artery making a lesser contribution. These are branches of the profunda femoris artery or deep femoral artery which in turn is a branch of the femoral artery. The labrum receives its vascular supply from the obturator and the superior and inferior gluteal arteries. Of note, labral tears are most likely to occur at the junction of the labrum and articular cartilage, an area that has been termed the ‘watershed region’. The head femur may also receive blood via an artery travelling through the ligamentum teres. There are two significant anastomoses, the cruciate anastomosis, supporting the thigh, and the trochanteric anastomosis, which supports the head of the femur.

Lymphatic drainage from the anterior aspect drains to the deep inguinal nodes, while the medial and posterior aspects drain into the internal iliac nodes. These nodes eventually drain to the paraaortic lymph nodes, which converge to form the right and left lumbar trunks then join the cisterna chyli. Some nodes, however, enter the preaortic and retroaortic lymph nodes, and others pierce the crura of the diaphragm to join the lower end of the thoracic duct.
The vascular and lymphatics systems of the body are important for both performance and regeneration. However, generally, they are viewed from a medical pathoanatomical perspective.
Wow! Again, that was a lot. Stayed tuned for Volume 2 where I will cover more SUP-specific hip mechanics…

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
5 thoughts on “SUP Biomechanics: Hips Volume 1”